Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 40 • Correction of Malrotation with Midgut Volvulus 419
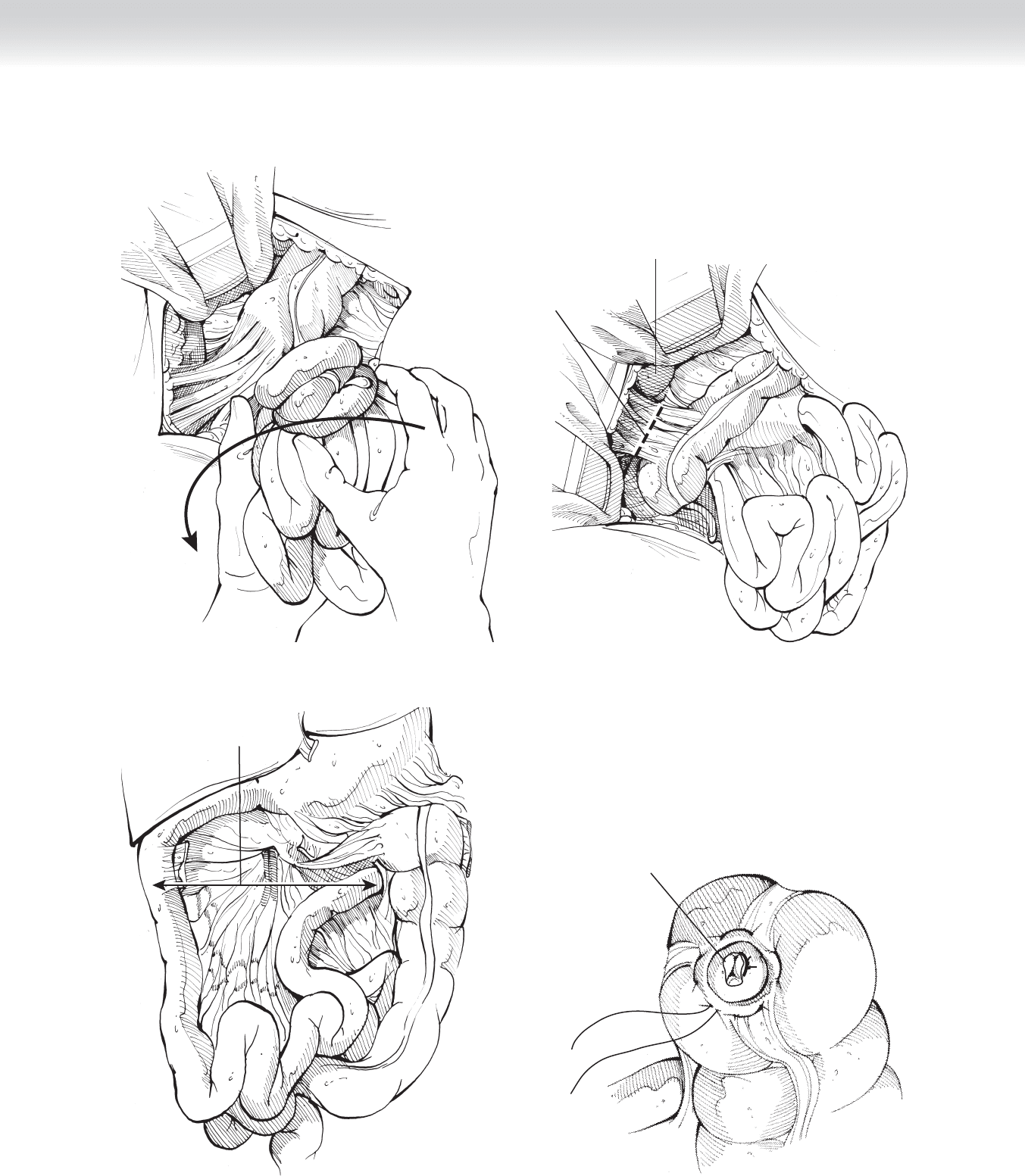
FIGURE 40 –5
Proposed
transection line
in Ladd's bands
Duodenum
FIGURE 40 –6
Broadened axis
FIGURE 40 –7
Appendiceal stump before
inversion
FIGURE 40 –8

420 Section IV • The Abdomen
3. CLOSING
◆ The incision is closed in layers with running 5-0 polyglactin sutures on tapered needles.
These layers include the peritoneum and posterior rectus fascia, anterior rectus fascia,
Scarpa’s fascia, and subcutaneous tissue. The skin is infi ltrated with 0.25% bupivacaine
without epinephrine and closed with a running 6-0 subcuticular absorbable undyed
monofi lament suture and adhesive strips.
STEP 4: POSTOPERATIVE CARE
◆ Continued monitoring in an intensive care setting and administering intravenous fl uids,
antibiotics, and analgesics are mandatory during the initial postoperative period. Prolonged
ileus or short bowel syndrome may require total parenteral nutrition. The incidence of
recurrent volvulus is less than 10%. Ladd’s procedure creates enough adhesions, broadens
the mesentery, and eliminates the fi xed point resulting from bands between the duodenum
and cecum so that recurrence of midgut volvulus is unlikely and seldom reported. The risk
of small bowel obstruction is not higher than that of any other open abdominal operations.
Wound infections or dehiscence are rare in cases in which no intestinal resections are
performed. Massive loss of bowel may lead to sepsis, septic shock, and death. In survivors,
short bowel syndrome results in dependency on total parenteral nutrition and ultimately
in small bowel or multiorgan transplantation.
STEP 5: PEARLS AND PITFALLS
◆ Great attention must be paid at the time of replacing the small bowel in the intestinal cavity.
It is very easy to kink or twist the intestinal blood supply, and any signs of venous conges-
tion or intestinal ischemia should prompt the surgeon to immediately exteriorize the bowel,
correct any twists or kinks of the mesentery, and resume the process of placing the intestines
in order back into the intestinal cavity.
SELECTED REFERENCES
1. Spitz L: Malrotation. In Spitz L, Coran AG (eds): Rob and Smith’s Operative Surgery (Pediatric Surgery),
5th ed. London, Chapman & Hall, 1995, pp 341-347.
2. Ashcraft K: Atlas of Pediatric Surgery. Philadelphia, Saunders, 1994, pp 97-101.

422
STEP 1: SURGICAL ANATOMY
◆ An understanding of the biliary and hepatic arterial anatomy is critical to performing suc-
cessful cholecystectomy (laparoscopic or open). The cystic duct joins the common hepatic
duct, forming the common bile duct distally. The cystic artery most commonly originates
from the right hepatic artery. However, there are many variants in both biliary and hepatic
arterial anatomy.
◆ To avoid common bile duct or hepatic arterial injury during cholecystectomy (laparoscopic
or open), it is necessary to identify the cystic duct at its origin from the infundibulum of
the gallbladder and to identify the cystic artery as it enters the gallbladder.
STEP 2: PREOPERATIVE CONSIDERATIONS
1. PREPARATION
◆ The indications for laparoscopic cholecystectomy include symptomatic cholelithiasis, acute
cholecystitis, chronic cholecystitis, biliary dyskinesia (low gallbladder ejection fraction), and
gallstone pancreatitis.
◆ Before induction of anesthesia, sequential compression devices should be placed on the lower
extremities and patients should be given subcutaneous heparin for venous thromboembolism
prophylaxis.
◆ The patient should be asked to void just before coming to the operating room. If this is not
done, a Foley catheter should be placed or a straight catheterization should be performed
for bladder decompression.
◆ A orogastric tube should be placed for decompression of the stomach.
CHAPTER
41
Laparoscopic and Open
Cholecystectomy
Taylor S. Riall

◆ A fi rst-generation cephalosporin should be used for antibiotic prophylaxis, unless the
patient is taking therapeutic antibiotics for acute cholecystitis. Clindamycin can be used
if the patient has a penicillin allergy.
2. OPERATING ROOM SETUP
◆ The patient is placed supine on the operating room table. Both arms can be out to the side,
or the left arm can be tucked.
◆ The surgeon stands on the patient’s left side, and the fi rst assistant stands on the patient’s
right side. If a second assistant is available to hold the camera, he or she stands on the
patient’s left side below the surgeon.
◆ The video monitors are arranged at the head of the bed on the right and left sides, such
that the surgeons and assistants can comfortably view the monitor across from them with-
out having to turn around.
◆ A fl uoroscopy table or table with x-ray capability is needed for possible intraoperative
cholangiography.
◆ For open cholecystectomy, the patient is supine with both arms extended.
CHAPTER 41 • Laparoscopic and Open Cholecystectomy 423

424 Section V • Gallbladder
STEP 3: OPERATIVE STEPS
LAPAROSCOPIC CHOLECYSTECTOMY
1. INCISION/PORT PLACEMENT
◆ The fi rst port is placed in the supraumbilical position. An 11-mm port is used (Figure 41-1).
◆ Access to the abdominal cavity can be performed using an open (Hasson) or closed (Veress
needle) technique.
◆ For either technique, the supraumbilical area is anesthetized with local anesthetic. A trans-
verse supraumbilical incision is made using a scalpel.
◆ For the open technique, electrocautery is used to dissect down to the fascia. The fascia is se-
cured with 0 Vicryl sutures, and the peritoneal cavity is opened under direct vision. The tro-
car is placed directly into the peritoneal cavity and secured with the 0 Vicryl sutures on each
side.
◆ For the closed technique, the Veress needle is inserted blindly into the abdominal cavity
after skin incision.
◆ The surgeons should observe free fl ow of fl uid into the needle to confi rm intraperitoneal
positioning.
◆ The initial pressure should be low (⬍3 mm Hg), confi rming intraperitoneal placement. The
abdomen is then insuffl ated to 15 mm Hg.
◆ The 11-mm trocar can then be placed under direct vision using a zero-degree laparoscope
and an optical port.
◆ After initial port placement, a 30-degree or zero-degree laparoscope can be used. The
30-degree scope can facilitate diffi cult views but requires a more experienced assistant.
◆ A 5-mm port is then placed in the right anterior axillary line along the costal margin,
between the 12th rib and the iliac crest (see Figure 41-1).
◆ A second 5-mm port is placed in the midclavicular line. Both of the 5-mm ports should
be 2 fi ngerbreadths below the right costal margin and should be 7 to 10 cm apart (see
Figure 41-1).
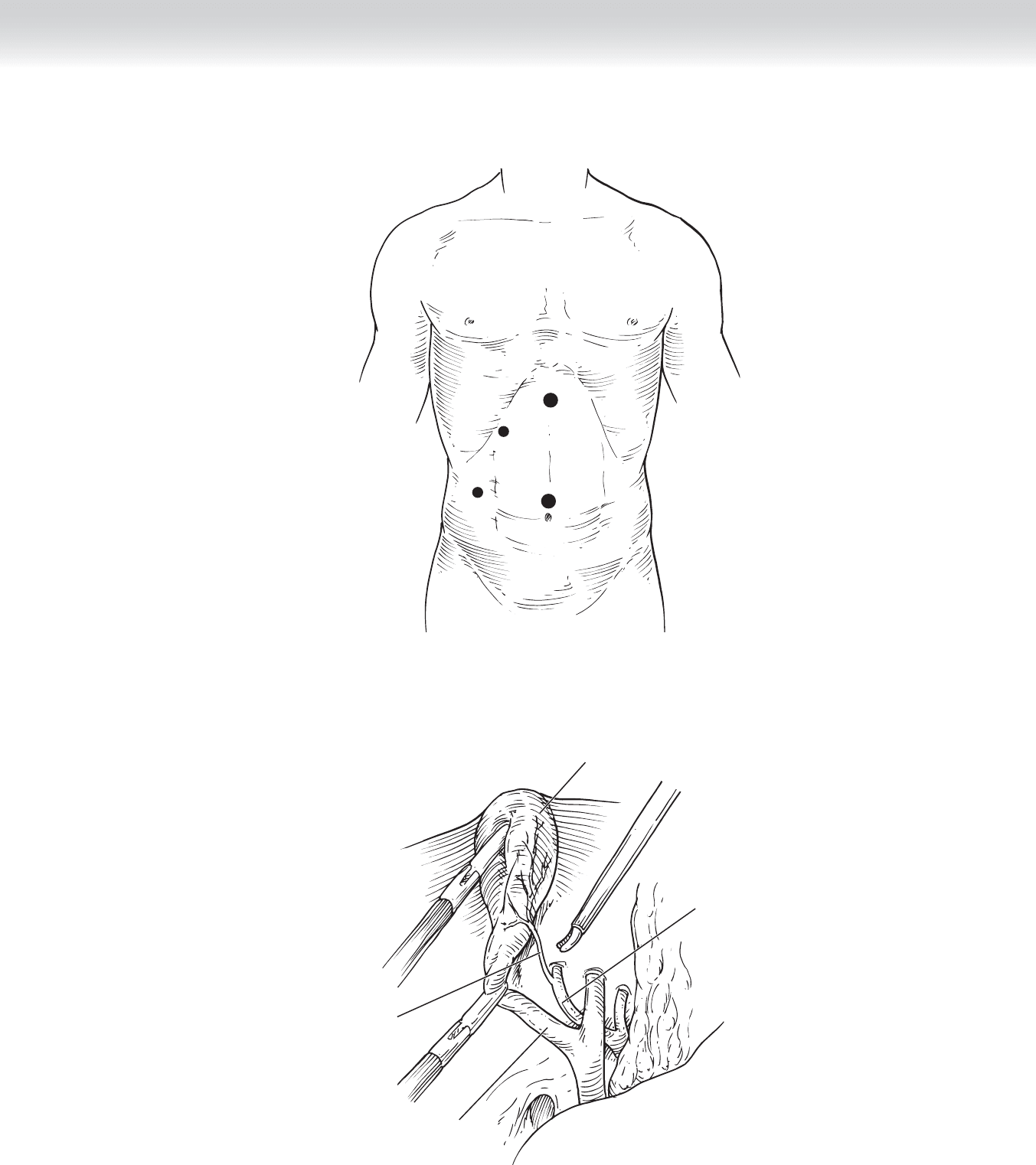
◆ The fi nal port is placed in the epigastric region (see Figure 41-1). This port should be placed
last and should be positioned after the gallbladder is retracted superiorly (Figure 41-2). This
allows the surgeon to place the port in a direct line to the infundibulum. This provides a
good line for clip placement and avoids unnecessary torque on the instruments.
CHAPTER 41 • Laparoscopic and Open Cholecystectomy 425
FIGURE 41 –1
Gallbladder
Cystic
duct
Cystic
artery
Right
hepatic
artery
FIGURE 41 –2

426 Section V • Gallbladder
2. DISSECTION
◆ The patient can be placed in reverse Trendelenburg position to allow the duodenum, stomach,
and other intra-abdominal contents to fall away from the dissection fi eld.
◆ A 5-mm locking grasper is placed through the most lateral port, and the gallbladder is
retracted cephalad, toward the patient’s right shoulder (see Figure 41-2).
◆ A second grasper is placed through the medial 5-mm port and used to retract the infundib-
ulum of the gallbladder laterally (to the patient’s right side) and inferiorly, opening up the
triangle of Calot (bounded by the cystic duct, the common hepatic duct, and the liver edge)
and better exposing the cystic structures (see Figure 41-2). This can be done by the fi rst
assistant or by the operating surgeon.
◆ Using a Maryland dissector through the epigastric port, any adhesions between the gallblad-
der and the omentum, hepatic fl exure, stomach, and duodenum are taken down by grasp-
ing them close to the gallbladder and peeling them down along the axis of the cystic duct.
◆ The dissection of the triangle of Calot is best performed laterally to medially, fi rst exposing
the infundibulum–cystic duct junction on the patient’s right side, then medially. The cystic
duct is circumferentially dissected (see Figure 41-2).
◆ The cystic artery, which is usually medial and superior with the infundibulum retracted
laterally, is then dissected circumferentially in similar fashion using the Maryland dissector
(see Figure 41-2).
◆ No structure should be divided until the cystic duct is identifi ed at the cystic duct–
infundibulum junction and the cystic artery has been identifi ed and dissected free.
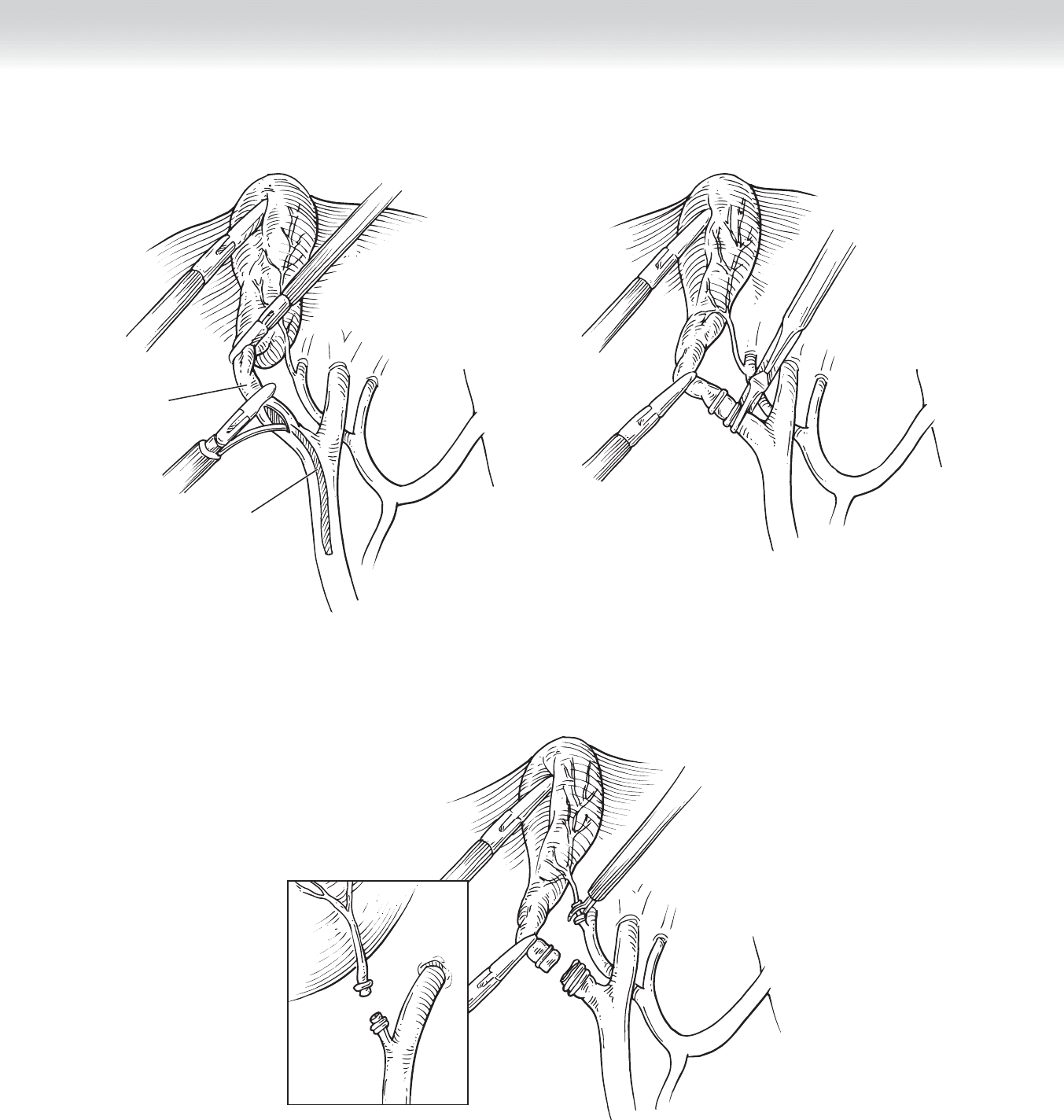
◆ At this point, cholangiography can be performed if indicated. Figure 41-3 demonstrates the
placement of a Kumar clamp through the 5-mm port. This clamp is placed entirely across
the cystic duct, occluding it and preventing fl ow of the contrast back into the gallbladder. A
cholangiocatheter with a needle tip is then placed through the clamp and into the cystic
duct distally. Contrast is injected, and a cholangiogram can be obtained to evaluate the bili-
ary anatomy and rule out any retained stones in the common bile duct.
◆ The cystic duct can now be ligated with clips applied with a 10-mm clip applier through
the epigastric port. Two clips should be placed distally and one proximally on the duct
(Figure 41-4).
◆ A curved or hook scissors is then used to divide between the most proximal and the two
distal clips (Figure 41-5).
CHAPTER 41 • Laparoscopic and Open Cholecystectomy 427
FIGURE 41 –5
FIGURE 41 –4
Cholangiocatheter
Cystic
duct
FIGURE 41 –3

428 Section V • Gallbladder
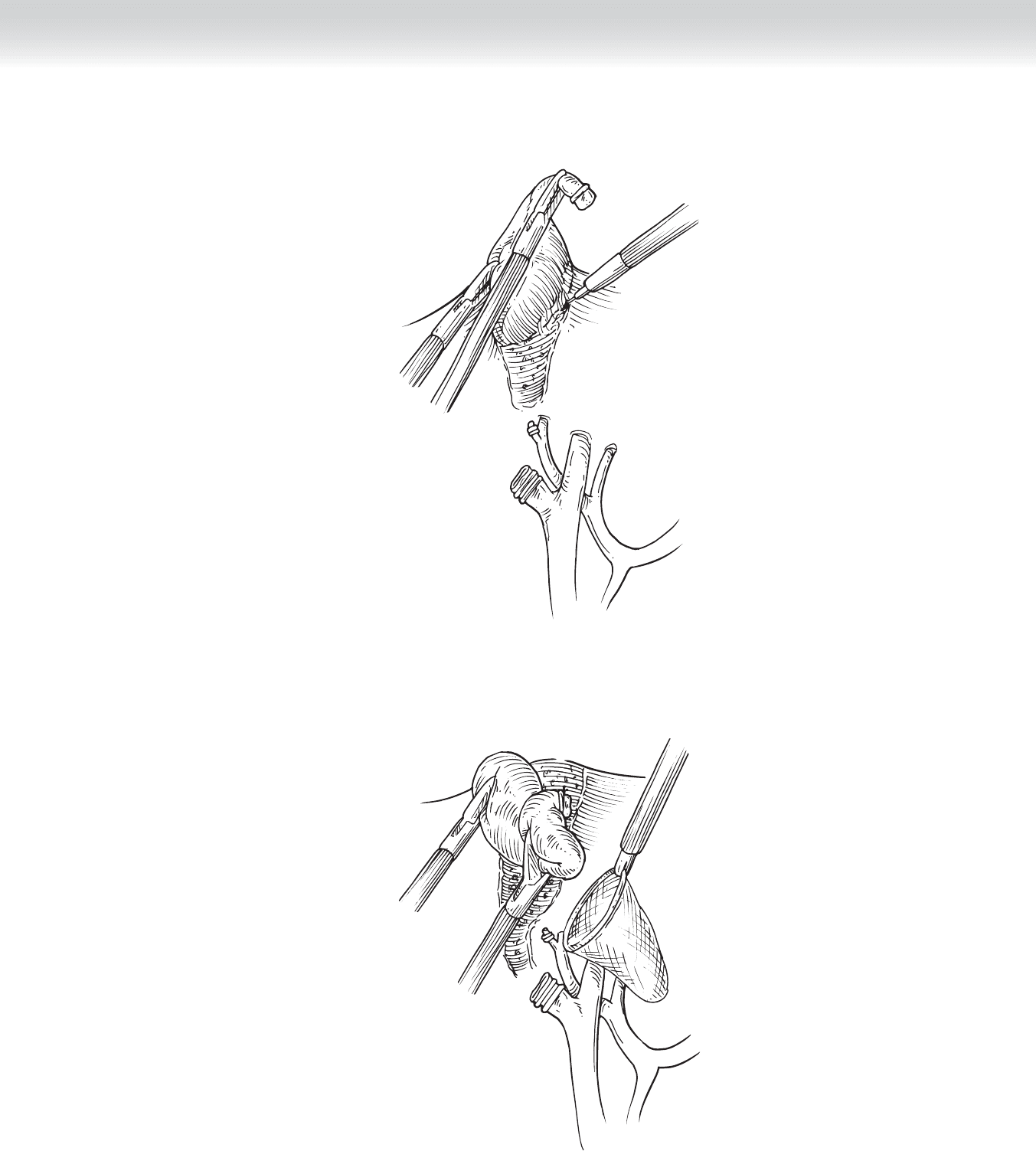
◆ The cystic artery is then clipped in similar fashion (see Figure 41-5) and divided with the
scissors, leaving two clips on the distal, retained stump.
◆ The gallbladder is then dissected out of the gallbladder fossa using electrocautery
(Figure 41-6). The hook cautery is shown here, but the dissection can also be performed
with a spatula, the Maryland dissector, or the scissors. This dissection is performed from
the infundibulum to the fundus. The graspers in the two 5-mm ports are used to provide
traction on the gallbladder, exposing the dissection plane between the gallbladder and
the liver.
◆ Before completely removing the gallbladder from the liver bed, the surgeon can use the
gallbladder to retract the liver while inspecting the cystic artery and duct stumps for any
signs of bleeding or bile leakage. Any bleeding from the liver bed should also be controlled
at this time.
◆ After removal of the gallbladder, the camera is placed through the epigastric port. A retrieval
bag is placed through the umbilical port (Figure 41-7). Removal with a retrieval bag is rec-
ommended especially if there is spillage of bile or gallstones.
◆ The gallbladder is placed in the retrieval bag (see Figure 41-7) and removed through the
umbilical port. The camera can then be replaced and the camera returned to the umbilical
port.
◆ The patient is returned to a fl at, supine position. The fi eld is then irrigated to ensure no
bleeding or bile leakage.
3. CLOSING
◆ The ports are removed under direct vision to make sure there is no bleeding from the port
sites.
◆ The fascia at the two 11-mm ports is usually closed with interrupted 0 Vicryl suture, which
can be placed using conventional methods or the laparoscopic suture passer. The fascia
at the 5-mm ports does not require closure.
◆ The skin is then closed with absorbable subcuticular sutures.
CHAPTER 41 • Laparoscopic and Open Cholecystectomy 429
FIGURE 41 –6
FIGURE 41 –7