Caballero B. (ed.) Encyclopaedia of Food Science, Food Technology and Nutrition. Ten-Volume Set
Подождите немного. Документ загружается.

relationship has not been established for many of
them. These include benzodiazepines, ciprofloxacin,
etomidate, enflurane, fluoxetine, furosemide, halo-
thane, interferon-a, isoniazid, maprotiline, meflo-
quine, nefazodone, octreotide, phenytoin, and
selegiline.
Alcohol
0019 Alcohol inhibits hepatic gluconeogenesis by depleting
nicotinamide adenine dinucleotide levels and by
decreasing the flux of gluconeogenic substrates (i.e.,
alanine, glycerol, lactate). However, it does not affect
glycogenolysis. Therefore, in the well-fed person,
hypoglycemia does not occur until after depletion of
glycogen stores by fasting > 12 h, along with con-
sumption of 50–300 g of alcohol during the preceding
6–36 h. In the poorly nourished individual, less alco-
hol may induce hypoglycemia more quickly. Alcohol
may also potentiate insulin and sulfonylurea-induced
hypoglycemia. Intravenous glucose causes prompt
recovery, unlike glucagon, which is ineffective. With-
out treatment, the mortality rate is 10% in adults and
25% in children.
Protein–Energy Malnutrition
0020 There are many descriptions of hypoglycemia in
severe protein–energy malnutrition (PEM), although
there seems to be no consistent difference in the
severity of hypoglycemia between marasmus and
kwashiorkor. The frequency of hypoglycemia varies
geographically, ranging from 10% in Jamaica to 24%
in Uganda. Hypoglycemia is a poor prognostic factor,
as its presence increases the mortality in marasmic
infants by 1.6–3.1-fold, unless intravenous glucose is
given immediately. The pathogenesis is not clear, but
high rates of glucose utilization in the presence of
total body fat depletion, limitation of substrate avail-
ability for gluconeogenesis, or diminished activity of
gluconeogenic enzymes are possibilities. Hypogly-
cemia is also seen in anorexia nervosa.
Endocrine Deficiencies
0021Endocrine deficiencies are rare causes of hypogly-
cemia. Deficiencies of cortisol and/or growth hor-
mone impair gluconeogenesis, especially in the very
young, or if other hypoglycemic stressors are present.
These endocrinopathies limit the availability of glu-
coneogenic substrate availability and decrease the
activity of hepatic gluconeogenic enzymes. Combined
deficiencies, e.g., in hypopituitarism, cause more
severe hypoglycemia. Isolated glucagon or epineph-
rine deficiencies in infants can also cause hypogly-
cemia but are extraordinarily rare. They can occur
as an acquired condition in individuals with long-
standing type 1 diabetes. Hypothyroidism can reduce
the rate of glucose absorption from the gut and
decrease peripheral glucose utilization. However, al-
though hypothyroidism has been said to be a cause of
hypoglycemia, it rarely occurs in isolated thyroxine
deficiency. The concurrence of hypoglycemia and
hypothyroidism should suggest the presence of ad-
renal insufficiency.
Severe Medical Illness
0022Severe liver disease, e.g., hepatectomy or fulminant
hepatitis can cause profound hypoglycemia, as the
liver is the major source of endogenous glucose
production. Renal failure is also associated with
hypoglycemia. Multiple mechanisms are involved,
including cachexia, uremic inhibition of hepatic
gluconeogenesis, failure of renal gluconeogenesis,
decreased renal clearance of insulin (in patients with
concurrent diabetes), and dialysis. Hypoglycemia
occasionally occurs in congestive heart failure,and
it is suggested that it is due to hepatic congestion,
cachexia, and inhibition of gluconeogenesis. Sepsis
increases peripheral glucose utilization and inhibits
hepatic gluconeogenesis, mediated by cytokines such
as tumor necrosis factor-a, interleukin-1, and inter-
leukin-6.
tbl0003 Table 3 Drugs associated with hypoglycemia
Drug Mechanism of inducing hypoglycemia
Insulin Increase glucose uptake by peripheral tissues
Sulfonylureas Increase insulin secretion via sulfonylurea receptors on b-cells
Pentamidine Increases insulin secretion
Quinine Increases insulin secretion
Salicylates Unknown mechanism – ? increase peripheral glucose uptake; need large doses (4–6 g)
Sulfonamides Unknown mechanism
Angiotensin-converting enzyme inhibitors ? Increases insulin sensitivity
Acetaminophen Hepatic necrosis in acute toxic overdoses
Disopyramide Increases insulin secretion
Monoamine oxidase inhibitors Unknown mechanism, rare
b-adrenergic antagonists ? Increase peripheral glucose uptake; ? inhibit gluconeogenesis; more common in
patients with diabetes
HYPOGLYCEMIA (HYPOGLYCAEMIA) 3209

Ackee Poisoning (Jamaican Vomiting Sickness)
0023 A toxic hypoglycemia syndrome occurs whenever the
unripe fruit of ackee (Blighida sapida) is consumed, as
first reported in 1875. Ackee was imported to the
New World from West Africa in 1778 and is found
in the Caribbean, Central America, and Florida.
Poisoning is more common in children, especially if
undernutrition is present. Adults generally have a
chronic course with a self-limited cholestatic jaun-
dice. The unripe arillus of the fruit contains hypo-
glycin, which is sequentially transaminated and
decarboxylated to methylenecyclopropylacetyl-CoA.
This metabolite irreversibly inhibits acyl-CoA dehy-
drogenases (especially butyryl-CoA dehydrogenase),
leading to inhibition of fatty acid b-oxidation. The
metabolic consequences are an acquired organic acid-
emia (mostly glutaric and ethylmalonic acid), the
absence of ketosis or hyperinsulinemia, and impair-
ment of hepatic gluconeogenesis. Patients have severe
hypoglycemia, an acute encephalopathy similar to
Reye’s syndrome, and severe vomiting. Convulsion,
coma and death can follow. Treatment involves inten-
sive glucose infusions to maintain normoglycemia.
Cooking renders the fruit nontoxic, reducing hypo-
glycin levels 100-fold.
Insulinomas
0024 Insulinomas are rare tumors with an incidence of four
cases per million person-years. Approximately 10%
are malignant, 9% are multifocal, 8% are recurrent,
and 8% occur as part of multiple endocrine neopla-
sia-1 syndrome. They are evently distributed through-
out the pancreas, and ectopic locations are unusual.
Some tumors cosecrete gastrin, adrenocorticotropic
hormone, glucagon, and 5-hydroxyindole. The diag-
nosis relies on documentation of Whipple’s triad with
inappropriately high insulin (36 pmol l
1
), C-pep-
tide (0.2 nmol l
1
), and proinsulin (5 pmol l
1
)
levels during hypoglycemia. Surreptitious use of ex-
ogenous insulin and sulfonylureas has to be ruled out,
and a 72-h supervised inpatient fast may be required
(Table 4). After biochemical confirmation, the tumor
may be localized by conventional, intraoperative, or
endoscopic ultrasonography. Magnetic resonance im-
aging or selective intraarterial injection of calcium
with venous sampling for insulin may be useful.
Some are localized by surgical exploration. Treatment
is by surgical enucleation of the tumor, and chemo-
therapy is necessary for palliation in individuals with
metastases.
Noninsulinoma Tumor-associated Hypoglycemia
0025There are various noninsulinoma tumors that
induce hypoglycemia, most commonly mesenchymal
cancers, hepatoma, adrenocortical carcinoma, lymph-
oma, and gastrointestinal cancers. Generally, hypo-
glycemia is a late presentation, the tumor burden is
large (> 500 g), and metastases are commonly present.
Many of these tumors produce insulin-like growth
factor-II as the putative hypoglycemic agent. They
rarely produce ectopic insulin. Occasionally, some
induce hypoglycemia by increasing glucose consump-
tion in excess of the liver’s gluconeogenetic ability.
Miscellaneous Causes
0026Factitious hypoglycemia is due to the surreptitious
use of insulin or sulfonylureas. This may be due to
malingering, Munchausen syndrome, attempted sui-
cide/homicide, or pharmacy error. A proper biochem-
ical evaluation during a 72-h fast (Table 4) should
reveal the diagnosis. Insulin levels > 1200 pmol l
1
should generate suspicion of factitious causes. Very
rarely, in patients naı
¨
ve to insulin, there may be a
spontaneous autoimmune antiinsulin antibody syn-
drome. This has been reported in Japanese patients
treated with thionamides or with other autoimmune
disorders. The mechanism involves an insulinomi-
metic action when the antiidiotypic antibodies to
antiinsulin antibodies interact with the insulin recep-
tor. An insulinomimetic action of antibodies against
the insulin receptor can cause hypoglycemia in type
B insulin resistance. Severe exercise, as seen in mara-
thon runners, has occasionally been associated with
hypoglycemia.
Childhood Hypoglycemia
0027As children have an increased ratio of brain to body
mass, they have higher rates of glucose flux. There is
also limited substrate availability for gluconeogenesis
due to their smaller muscle mass. Hence, they are not
tbl0004 Table 4 Interpretation of the results of a 72-h fast
Diagnosis Insulin C-peptide Proinsulin Plasma or urine sulfonylurea b-Hydroxybutyrate
Insulinoma Increased Increased Increased Negative None
Exogenous insulin Increased Decreased Decreased Negative None
Sulfonylurea ingestion Increased Increased Increased Present None
Noninsulin-mediated hypoglycemia Decreased Decreased Decreased Negative Increased
3210 HYPOGLYCEMIA (HYPOGLYCAEMIA)

able to tolerate hypoglycemia as easily as adults.
Their clinical presentation is more variable with
hypotonia, cyanosis, hypothermia, tachypnea, feed-
ing difficulties, and poor neuropsychiatric develop-
ment being prominent. Older children have more
adrenergic symptoms and may have focal neuro-
logical deficits and movement disorders.
0028 Most of the causes of hypoglycemia in adults are
also seen in children. Transient hyperinsulinism is the
most frequent cause of hypoglycemia in the infant, as
seen in the children of diabetic mothers, premature
infants, and small-for-gestational-age infants. Con-
genital hyperinsulinism, otherwise called nesidioblas-
tosis or persistent hyperinsulinemic hypoglycemia of
infancy, describes diffuse b-cell hyperplasia with
hyperinsulinemic hypoglycemia. Subtotal pancrea-
tectomy or medical treatment with diazoxide or
octreotide is advocated for symptomatic infants.
This is due to genetic mutations that affect the normal
intracellular events controlling insulin secretion. The
mutations include:
.
0029 mutations inactivating the ATP-sensitive potassium
channel in b-cells leading to membrane depolariza-
tion (SUR1 and Kir6.2 subunit mutations);
.
0030 activating mutations of the glucokinase gene
increasing glycolysis; and
.
0031 activating mutations of the glutamate dehydrogen-
ase gene causing an increased rate of glutamate
oxidation in b-cells (hyperinsulinism/hyperammo-
nemia syndrome, which includes leucine-sensitive
hypoglycemia, as leucine is an allosteric activator
of GDH and thus functions as an insulin secret-
agogue).
Hypoglycemia is also a consequence of inborn errors
of metabolism involving gluconeogenesis, glycogen
storage, fatty acid metabolism, and amino acid
metabolism.
0032 Ketotic hypoglycemia of childhood generally
begins between the ages of 1.5 and 5 years, and
resolves by age 10. It probably accounts for 90% of
children with hypoglycemia beyond infancy, and it
may represent a subset of children who are least
tolerant of fasting, especially during an intercurrent
illness. These children characteristically have rela-
tively decreased muscle mass, and there may be
a defect in mobilizing alanine for gluconeogenesis.
Although alanine administration increases blood
glucose levels, treatment generally involves avoiding
any prolonged fasting.
See also: Alcohol: Properties and Determination;
Diabetes Mellitus: Etiology; Problems in Treatment;
Glucose: Properties and Analysis; Function and
Metabolism; Maintenance of Blood Glucose Level;
Glucose Tolerance and the Glycemic (Glycaemic) Index;
Hormones: Pituitary Hormones; Malnutrition: The
Problem of Malnutrition
Further Reading
Bolli GB (1999) How to ameliorate the problem of hypo-
glycemia in intensive as well as nonintensive treatment
of type 1 diabetes. Diabetes Care 22 (supplement 2):
B43–B52.
Cryer PE (1997) Hypoglycemia: Pathophysiology, Diagno-
sis and Treatment. New York: Oxford University Press.
Haymond MW and Pagliara AS (1983) Ketotic hypo-
glycemia. Clinical Endocrinology and Metabolism 12:
447–462.
Hofeldt FD (1989) Reactive hypoglycemia. Endocrinology
and Metabolism Clinics of North America 18: 185–201.
Malouf R and Brust JCM (1985) Hypoglycemia: causes,
neurological manifestations and outcome. Annals of
Neurology 17: 421–430.
Marks V (1987) Functional hypoglycemia: fact or fancy. In:
Andreani D, Marks V and Lefebvre PJ (eds) Hypo-
glycemia: Serono Symposium, vol. 38, pp. 1–17. New
York: Raven Press.
Seltzer HS (1989) Drug-induced hypoglycemia. Endocrin-
ology and Metabolism Clinics of North America 18:
163–183.
Service FJ (1995) Hypoglycemic disorders. New England
Journal of Medicine 332: 1144–1152.
Service FJ (ed.) (1999) Hypoglycemic disorders. Endocrin-
ology Clinics of North America vol. 28(3). Philadelphia,
PA: W.B. Saunders.
Sovik O (1989) Inborn errors of amino acid and fatty
acid metabolism with hypoglycemia as a major clinical
manifestation. Acta Paediatrica Scandinavica 78:
161–170.
Sperling MA and Menon RK (1989) Hyperinsulinemic
hypoglycemia of infancy. Recent insights into ATP-
sensitive potassium channels, sulfonylurea receptors,
molecular mechanisms, and treatment. Endocrinology
and Metabolism Clinics of North America 28: 695–708.
Tanaka K and Ikeda Y (1990) Hypoglycin and Jamaican
vomiting sickness. Progress in Clinical and Biological
Research 321: 167–184.
HYPOGLYCEMIA (HYPOGLYCAEMIA) 3211
HYPOVITAMINOSIS A
V Reddy, Panjagutta, Hyderabad, India
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Introduction
0001 Vitamin A is an essential nutrient required for normal
vision, growth, and development, maintenance of
epithelial cellular integrity, immune response, and a
variety of metabolic functions. It is a fat-soluble vita-
min and is stored in the body when intake exceeds
need. Depletion of stores occurs over time when the
diet does not provide enough vitamin A to replace the
amount used by the tissues. Signs of hypovitaminosis
A appear when the stores are depleted to the extent
that physiological functions are impaired. A series of
problems ranging from ocular changes to growth
retardation and increased mortality have been docu-
mented in vitamin A-deficient animals, while in
human vitamin A deficiency (VAD), attention is
focused on xerophthalmia because of the striking
changes in the eye. VAD is recognized as the most
important cause of childhood blindness in developing
countries. Apart from causing eye damage, VAD can
also affect host defense mechanisms, increasing sus-
ceptibility to infection. There is evidence that VAD,
even at subclinical level, increases the risk of morbid-
ity and mortality in vulnerable groups. Recognizing
the importance of the problem, heads of state and
other high-level policy makers gathered at the World
Summit for Children (1990) and the International
Conference on Nutrition (1992) adopted the goal
of elimination of VAD by the year 2000. Although
considerable progress has been made in the past
decade, VAD remains a public health problem in
many developing countries. There is a need to accel-
erate the intervention efforts to eliminate VAD and its
consequences.
Dietary Sources of Vitamin A
0002 Vitamin A is obtained through the diet as preform-
ed vitamin A or provitamin A carotenoids. Preformed
vitamin A is present in animal foods such as milk,
butter, eggs, liver, and fish. In most tropical countries,
where consumption of these foods is low, the main
sources of vitamin A in the diet are the provitamin A
carotenoids. These are present in dark-green leafy
vegetables, yellow/orange vegetables like carrots and
pumpkin, and fruits like mango and papaya. Red
palm oil, used mostly in African countries, has a
very high concentration of b-carotene. Of the various
carotenoids in foods, b-carotene has the maximum
vitamin A activity. Other provitamin A carotenoids
include a-carotene and b-cryptoxanthine, which
have approximately half the vitamin A activity of
b-carotene. Values of carotene/vitamin A given in
most food composition tables are overestimates, as
they are based on old analytical methods which do
not distinguish between provitamin A and other
carotenoids. Only recently have accurate values for
provitamin A carotenoids been obtained, using high-
performance liquid chromatography (HPLC)
technique.
Recommended Dietary Intakes
0003The recommended intakes of vitamin A for different
age groups are given in Table 1. These intakes are
designed to prevent deficiency and provide a safe
intake for a majority of the population. The values
are expressed in terms of retinol equivalents (RE) per
day, taking into account vitamin A activity of provi-
tamin A carotenoids. The Food and Agriculture Or-
ganization/World Health Organization (FAO/WHO)
expert committee has suggested a ratio of 6:1 for
converting b-carotene to vitamin A, assuming that
one-third of the carotene in the diet is absorbed and
half of it is converted to vitamin A. However, recent
studies showed lower bioavailability of carotene,
with a ratio of 26:1 for vegetables and 12:1 for fruits.
Bioavailability of dietary carotenoids is influenced by
a number of factors, including the food source,
method of preparation, amount ingested, and dietary
fat. Any single/average ratio for the conversion of
carotenoids to vitamin A is at best a rough estimate
that is not valid for all diets.
tbl0001Table 1 Recommended dietary intake of vitamin A
Group Age
(years)
Recommended intake
(mgREday
1
)
Both sexes 0–1 350
1–10 400
10–12 500
12–15 600
Boys 15–18 600
Men 18þ 600
Girls 15–18 600
Women 18þ 500
Pregnant women 600
Lactating women 850
RE, retinol equivalent.
Reproduced from FAO/WHO Consultation (1998) Requirements of Vitamin A,
Iron, Folate and Vitamin B
12
, pp. 16–31. Rome: FAO, with permission.
3212 HYPOVITAMINOSIS A

Assessment of VAD
0004 Several methods are available for assessing the
magnitude and severity of VAD in a population.
These include clinical, functional, and biochemical
indicators. The WHO monograph on indicators of
VAD provides guidelines on the selection and
interpretation of practical indicators for population
assessment.
Clinical Indicators
0005 Clinical indicators are useful for assessing the extent
of VAD in communities where clinical problem or
xerophthalmia exists. The core indicators and the
minimum prevalence criteria to define a public
health problem are given in Table 2. Corneal xero-
phthalmia indicates a serious problem but the
condition is relatively rare and requires a large
sample size to estimate the prevalence. Night
blindness (XN) and Bitot’s spots (X1B) are the two
indicators commonly used in community surveys.
Conjunctival xerosis is not a reliable sign, while xero-
sis with Bitot’s spot is more specific and a prevalence
above 5% in preschool children indicates a public
health problem.
Indicators of Subclinical Deficiency
0006 Serum retinol is the most commonly used biochem-
ical indicator. Values < 0.70 mmol l
1
are considered
as indicative of VAD in children. The cut-off levels of
prevalence used for defining a public health problem
of moderate to severe degree are shown in Table 3.It
is possible to estimate retinol concentration in finger-
prick blood samples using a filter paper technique,
which offers logistic advantages. Other indicators
include relative dose response (RDR) test for
assessing vitamin A stores and conjunctival impres-
sion cytology (CIC) for detection of conjunctival
changes that precede clinical signs. However, these
tests have limited application in field surveys.
Global Prevalence
0007Earlier estimates of VAD prevalence were based on
clinical signs of xerophthalmia, while more recent
surveys include data on subclinical deficiency based
on blood levels of vitamin A < 0.70 mmol l
1
.Itis
now estimated that VAD, including clinical and sub-
clinical forms of moderate to severe degrees of public
health significance, exists in 60 countries and it is
likely to be a problem in at least an additional 13
countries. On a regional basis, South-east Asia and
Africa account for just under 90% of the global prob-
lem (Figure 1). Although the prevalence of clinical
deficiency has shown a marked decline from 14 mil-
lion in 1994 to 3 million in 1996, estimates of
subclinical deficiency have gone up to 251 million,
with the increasing use of serum retinol concentration
for assessment. About 254 million children in the
world are thus at risk in terms of their health and
survival.
Epidemiology
Socioeconomic Factors
0008VAD occurs within an ambience of ecological, eco-
nomical, and social deprivations that characterize the
poor in developing countries. At the macro level,
adverse environment with infertile land and water
shortage limit the availability of foods rich in
vitamin A. Since animal foods containing prefor-
med vitamin A are expensive, poor families rely on
plant sources of provitamin A carotenoids. Illiterate
and impoverished mothers tend to follow traditional
feeding practices and do not fully utilize even the
available resources. High infection rates associated
with poor living conditions also contribute to hypo-
vitaminosis A.
Clustering
0009The occurrence of VAD tends to cluster rather than
to be evenly distributed. Clustering within high-risk
households and within communities has been de-
scribed primarily for clinical deficiency. Studies in
Asia show that siblings of xerophthalmic children
are 10 times more likely to have xerophthalmia than
tbl0002 Table 2 Classification of xerophthalmia and prevalence
criteria constituting a public health problem
Criteria Minimum prevalence
Night blindness (XN) > 1.0%
Bitot’s spots (X1B) > 0.5%
Corneal xerosis/ulceration > 0.01%
(X2, X3A, X3B)
Corneal scar (XS) > 0.05%
Data from: WHO (1995) Global Prevalence of Vitamin A Deficiency. Geneva:
WHO, with permission.
tbl0003 Table 3 Classification of subclinical deficiency (serum retinol
< 0.70 mmol l
1
)
Public health problem Prevalence inchildren
Mild 2–< 10%
Moderate 10–< 20%
Severe 20%
Data from: WHO (1995) Global Prevalence of Vitamin A Deficiency. Geneva:
WHO, with permission.
HYPOVITAMINOSIS A 3213
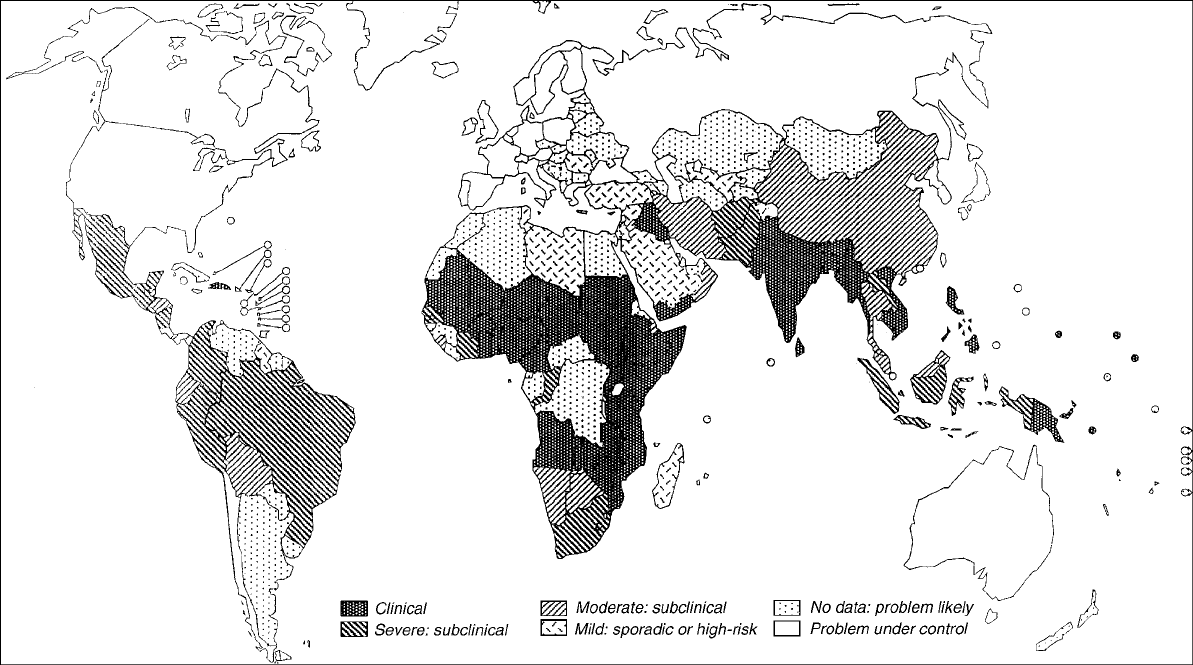
fig0001 Figure 1 Global prevalence of vitamin A deficiency. Reproduced from WHO (1995) Global Prevalence of Vitamin A Deficiency. Micronutrient Deficiency Information System. Working Paper #2.
WHO/NUT/95.3. Geneva: WHO, with permission.

those without. Neighboring children of xeroph-
thalmic children are also more likely to develop
xerophthalmia. This is due to sharing common socio-
cultural and economic conditions that result in fre-
quent infections, limited food availability, and poor
dietary practices that predispose to VAD.
Seasonal Patterns
0010 The occurrence of xerophthalmia follows a seasonal
pattern in different parts of the world. In South Asia,
for example, a distinct peak in the incidence of xer-
ophthalmia is observed in the month of May–June.
The peak appears to be related to the total food intake
and consequent growth spurt of children. It also coin-
cides with a general scarcity of provitamin A-rich
vegetables and fruits and a seasonal rise in the
incidence of diarrhea and respiratory infection.
Host Factors
0011 Age VAD is more common among children of pre-
school age. While xerophthalmia rarely occurs during
infancy, children between 1 and 4 years are at greater
risk. The potentially blinding corneal disease is most
prevalent during the weaning period and is associated
with severe protein-energy malnutrition (PEM).
Symptoms of milder xerophthalmia like Bitot spots
and night blindness are more common in older chil-
dren. Hypovitaminosis A persists throughout adoles-
cence and into adulthood, as judged by low serum
retinol levels. Clinical signs of xerophthalmia are rare
in adults except for maternal night blindness. Reports
from Asia indicate that about 10–20% of women
develop night blindness during pregnancy.
0012 Sex No consistent sex difference is demonstrated
based on physiological parameters. Differences have
been reported in some communities, which are more
likely to be related to sex differences in cultural prac-
tices of feeding and care rather than to physiological
differences.
Dietary Practices
0013 In poor communities, diets are deficient in several
nutrients, including vitamin A. Pregnant and lactating
women rarely take any extra food to meet their add-
itional needs. As a result, the offspring are born with
poor stores of vitamin A. During the first 6 months of
life, breast milk is the major source of vitamin A for
infants but the vitamin concentration of milk is low in
undernourished mothers. Although clinical signs of
VAD are rare in infants, their vitamin stores are de-
pleted. Complementary feeding is delayed and foods
rich in vitamin A are seldom given, increasing the risk
of VAD during the weaning period. Diet surveys in
countries of South Asia show that the daily intake of
vitamin A among preschool children is less than half
the recommended intake and most of it is derived
from plant sources of provitamin A carotenoids.
Bioavailability of plant carotenoids is low and it is
difficult to meet the needs of young children from
vegetable foods alone. Dietary fat is important for
the absorption of carotenoids but the weaning diets
contain little fat. These patterns signal the need to
improve child feeding practices in high-risk families
to sustain adequate vitamin A status.
Protein-Energy Malnutrition
0014VAD is often associated with protein-energy malnu-
trition (PEM) in children. Clinical studies show that
the prevalence of xerophthalmia is higher in children
with PEM than in those without. Almost all cases of
corneal xerophthalmia/keratomalacia are associated
with severe PEM. These observations suggest that
protein deficiency may aggravate VAD (often associ-
ated with protein-energy malnutrition in children).
Experimental studies show that there is a close
metabolic relationship between protein and vitamin
A. While the synthesis of retinol-binding protein
(RBP) that carries vitamin A is influenced by protein
nutrition, its release from the liver depends on vita-
min A status. Studies in malnourished children with
corneal xerophthalmia have shown that the concen-
tration of serum retinol was reduced to a greater
extent than that of RBP. Administration of vitamin
A to such children not only raised serum levels of
these components but also showed a rapid clinical
improvement. These observations indicate that the
role of vitamin A is more critical than that of protein
in the development of corneal lesions. Appreciation
of this fact has an important bearing on the treatment
and prevention of xerophthalmia.
Infections
0015Keratomalacia is often preceded by an episode of
infection: diarrhea and respiratory infection are
common precipitating factors. Prospective studies
also show that common childhood infections,
including diarrhea, respiratory illness, measles, and
chickenpox, induce hypovitaminosis A. During acute
infection, not only is the food intake reduced but
metabolic alterations are also known to occur. These
include decreased absorption of vitamin A, impaired
retinol transport, and increased renal excretion. Slow
normalization of these mechanisms coupled with low
dietary intake of vitamin A during the acute phase
and recovery lead to VAD. Parasitic infections like
ascariasis and giardiasis also aggravate VAD. Intes-
tinal worms may directly compete for uptake of
HYPOVITAMINOSIS A 3215

vitamin A, besides their more general impact on
health by suppressing appetite.
Xerophthalmia
0016 Although hypovitaminosis A affects many tissues in
the body, the most striking changes are seen in the
eye. The conjunctival and corneal epithelium undergo
keratinizing metaplasia. Columnar epithelial cells
become squamous and mucus-producing goblet
cells disappear, resulting in dryness/xerosis of the
ocular surfaces. Hypovitaminosis A also affects
the retinal function. Vitamin A is required for the
synthesis of rhodopsin, a photosensitive pigment in
the rod cells of retina that responds to light by releas-
ing vitamin A. If the vitamin is not replaced, rhodop-
sin production is reduced, resulting in impaired dark
adaptation and night blindness.
Night Blindness
0017 Night blindness is one of the early manifestations of
VAD and is marked by an inability to move around in
the dark. It is common among pregnant women
in endemic areas and often disappears after delivery
without any treatment. Night blindness is also
common among preschool children but its detection
is difficult in children below 2 years. In endemic
areas, a local term is often used for night blindness
that translates into ‘twilight blindness’ or ‘chicken
eyes’ (chicken have no rods and are therefore night-
blind), making the condition readily detectable by
history. Impaired dark adaptation is an early func-
tional abnormality which can be detected using a
dark adaptometer.
Conjunctival Changes
0018 Conjunctival xerosis appears as a dry, unwettable
surface of the bulbar conjunctiva. The conjunctival
changes that precede clinical signs can be detected
by filter-paper impression cytology. These include
keratinization/distortion of epithelial cells and disap-
pearance of goblet cells. In chronic cases, accumula-
tion of keratinized cells appears as white foamy
patches of oval or triangular shape called Bitot’s
spots. They are usually bilateral and seen on the
temporal side of the corneal limbus.
Corneal Changes
0019 Severe deficiency of vitamin A involves the cornea,
affecting the vision. The earliest corneal epithelial
changes appear as punctate defects, which can be
detected by a slit lamp. Clinically, the cornea appears
dry, hazy, and lusterless (X2). In severe cases, corneal
ulcers (X3A) appear as round or oval defects that
are usually shallow, but may progress to perforation
of cornea. Healed ulcers appear as white scars (XS)
and affect vision if they are centrally located. In
more advanced cases, there is necrosis and softening
of cornea (X3B). This condition, described as kera-
tomalacia, often results in permanent blindness.
Corneal xerophthalmia is invariably associated
with severe PEM and infection. Hospital studies
show high mortality in such cases, ranging from 5
to 25%.
Mortality
Childhood Mortality
0020Preschool age Vitamin A has been named as ‘anti-
infective vitamin’ as early as 1928, based on the evi-
dence obtained from animal studies. Although there
were several reports on the association of xerophthal-
mia with increased mortality among malnourished
children during the subsequent years, the importance
of vitamin A in child health and survival was not fully
recognized until late 1980s. Community studies in
Indonesia showed that preschool children with mild
xerophthalmia were two to three times more likely to
have developed diarrhea and respiratory illness than
those with normal eyes. The risk of mortality was also
higher in such cases. The effect of VAD on infection
may be mediated through several mechanisms, in-
cluding impairment of mucosal epithelial barrier
and of the immune response. Low T-cell count and
impaired blast transformation have been reported in
vitamin A-deficient children.
0021An intervention trial conducted in Indonesia
showed that administration of 6-monthly doses of
200 000 IU vitamin A to preschool children resulted
in 34% reduction in mortality. This stimulated a lot
of interest worldwide and led to a series of field trials
in Asia and Africa. Six out of eight controlled trials in
children showed mortality reductions ranging
from 19% to 54%. However, two studies reported
from India and Sudan showed no significant impact.
Metaanalysis of data from these studies has estimated
a reduction of total mortality by 30%.
0022Thus, vitamin A supplementation has resulted in
significant reductions in mortality in several, though
not all, community studies. Vitamin A had a protect-
ive effect against death from measles and diarrhea but
not from respiratory infection. The impact of vitamin
A may vary in different situations depending upon the
extent and severity of VAD, existence of concomitant
nutritional deficiencies, particularly PEM, and the
prevalence of infections in the community. The sup-
plements are expected to have a greater impact in
areas where VAD is highly prevalent.
3216 HYPOVITAMINOSIS A

0023 Early infancy A few studies have examined the effi-
cacy of vitamin A supplementation among apparently
normal infants under 6 months of age. Administra-
tion of a single dose of 50 000 IU vitamin A to neo-
nates in Indonesia resulted in a significant reduction
in the risk of death while no effect was observed in a
similar study in Nepal. Similarly, in a multicentric
WHO study conducted in India, Peru and Ghana,
administration of three doses of vitamin A along
with diphtheria, pertussis, typhoid (DPT) vaccine in
the first 4 months of age had no effect on infant
mortality or morbidity.
0024 Measles-related mortality Beneficial effect of vita-
min A on measles-related morbidity and mortality in
children was reported as early as 1932. In recent
placebo-controlled hospital studies conducted in
South Africa and Tanzania, administration of large
doses of vitamin A to children on admission for severe
measles resulted in a 60% reduction in case fatality.
The mortality reduction was higher (70%) when
measles was associated with pneumonia. The protect-
ive effect of the supplements was apparently greater
among infants than in older children.
Pregnancy-Related Mortality
0025 Although several studies have examined the impact of
vitamin A on child survival, maternal health has not
received much attention. Recently, a community trial
conducted in Nepal showed that weekly supplements
of vitamin A or b-carotene reduced pregnancy-related
mortality (mortality during pregnancy up to 12 weeks
postpartum). However, differences were only signifi-
cant when the two groups were pooled. It is surpris-
ing to note that the carotene group with lower retinol
concentration showed a greater reduction in mortal-
ity than the vitamin A group. Furthermore, supple-
mentation was associated with protection from
deaths due to injuries and miscellaneous causes but
had no impact on mortality ascribable to infections
and obstetric causes. Further studies are under way to
determine the role of vitamin A in maternal health
and survival.
Morbidity
0026 Unlike the impact on mortality, the effects of vitamin
A on morbidity have been more difficult to establish.
This may be due to variation in disease sensitivity to
vitamin A and inherent problems in assessing the
prevalence and severity of morbidity. Vitamin A
does not have much effect on the prevalence of
common childhood diseases but it appears to reduce
the severity of potentially fatal infections such as
measles, persistent diarrhea, and malaria, especially
in the presence of wasting malnutrition. The protect-
ive effect becomes stronger with the episode severity.
In Bangladesh, administration of vitamin A had no
impact on the duration of illness or stool output in
children with watery diarrhea, although children
with shigellosis who received vitamin A supplements
were 32% less likely to be clinically ill as compared
to placebo group. In Ghana, vitamin A supplemen-
tation was associated with fewer or less severe com-
plications and reduced rates of hospitalization for
severe measles. However, vitamin A has no effect on
nonmeasles respiratory disease. In some cases, sup-
plementation was associated with an increased risk of
lower respiratory infection. This appears a paradox,
considering the beneficial effect of vitamin A on the
epithelial structures.
0027Recent studies suggest that vitamin A may have
a role in other infections, particularly human
immunodeficiency virus (HIV) infection. In adults,
low plasma vitamin A concentration was associated
with increased clinical progress of HIV infection and
greater mortality. It was also found that low vitamin
A concentration during pregnancy was associated
with increased transmission of infection from mother
to child and also increased infant mortality. However,
clinical trials in South Africa and Tanzania showed
that vitamin A supplementation during pregnancy
had no effect on vertical transmission of the disease.
In another study, vitamin A supplements reduced
diarrheal morbidity in HIV-infected infants. Further
research is needed to explore the role of vitamin A in
HIV infection.
Treatment of Xerophthalmia
0028All individuals with xerophthalmia (except pregnant
women) should be treated with large oral doses of
200 000 IU vitamin A according to the WHO guide-
lines (Table 4). The age-specific dose should be given
on the first and second days and again 2 weeks later.
This applies to all stages of active xerophthalmia,
including night blindness, Bitot’s spots, and corneal
lesions. Corneal xerophthalmia is a medical emer-
gency and should be treated immediately on diagnosis
and then patients should be referred to a hospital
tbl0004Table 4 Treatment of xerophthalmia
Age (months) Dose of vitaminA (IU)
< 6 50 000
6 – 12 100 000
> 12 200 000
Three doses: on diagnosis þnext day þ2 weeks later.
HYPOVITAMINOSIS A 3217

for further treatment as they often present complex
problems. Topical application of antibiotic ointment
(tetracycline or chloramphenicol) is recommended
for corneal lesions to prevent secondary infection. In
addition, patients should be provided nutritional
support and medical therapy.
0029 Corneal xerosis shows improvement within a
week but in more advanced cases (corneal ulcer/
keratomalacia), healed scars remain as white opaci-
ties, resulting in partial or total blindness. Night
blindness responds in a couple of days while Bitot’s
spots take 3–10 days and some may persist, particu-
larly in older age groups.
0030 Pregnant women should be treated with small
doses of vitamin A, not exceeding 10 000 IU daily or
25 000 IU weekly, for about a month. Large doses of
vitamin A should be avoided during pregnancy to
avoid the risk of teratogenicity.
Prevention of VAD
0031 Inadequate dietary intake of vitamin A is the primary
cause of VAD and therefore the most rational ap-
proach to prevent the condition would be to improve
the diet and increase the intake of vitamin A. As a
short-term measure, however, vitamin A supplemen-
tation of the high-risk groups is suggested for provid-
ing immediate relief. Food fortification is also an
effective way of increasing vitamin A intake in the
population.
Vitamin A Supplementation
0032 Since vitamin A can be stored in the liver, periodic
administration of large doses of vitamin A has been
recommended for prevention of VAD. Children be-
tween 1 and 6 years of age are given an oral dose of
200 000 IU vitamin A every 4–6 months, while those
between 6 and 12 months are given half the dose.
Large-scale supplementation programs are now
in operation in many developing countries where
VAD is a major public health problem. Universal
distribution, involving administration of the dose to
all preschool children, is adopted by most countries.
In addition, targeted distribution of vitamin A is
recommended for the high-risk groups (severe
PEM, measles, siblings of children with xerophthal-
mia). Even in areas where a vitamin A program is in
operation, these children can be given an additional
dose of vitamin A if they had not received the supple-
ment in the previous month.
0033 Although vitamin A supplementation is widely im-
plemented, the coverage is inadequate in most areas.
It has been suggested that supplementation may be
linked with the national immunization program to
take advantage of immunization contacts for the de-
livery of vitamin A. In most national programs, the
first dose of vitamin A is given along with measles
vaccine at the age of 9 months. In Bangladesh, vita-
min A supplements are given earlier along with DPT
immunization. A higher incidence of side-effects like
nausea, vomiting, and bulging fontanel were ob-
served with this regimen, raising concern about sup-
plementation in early infancy. However, the
symptoms were mild and transient, disappearing
within 48 h and follow-up studies showed no long-
term sequelae. A WHO multicentric study conducted
more recently confirmed the safety of vitamin A sup-
plements but this regimen had no significant benefit
for the infants.
0034Administration of a large dose of 200 000 IU vita-
min A has been recommended for lactating mothers
within 8 weeks of delivery to raise vitamin A concen-
tration of milk and thus improve vitamin A status of
the infant. However, recent studies show that the dose
is not enough to produce any beneficial effect. In-
creasing the amount of vitamin A (two doses of
200 000 IU each) has been suggested. Further studies
are needed to determine the feasibility and safety of
administering two large doses within 8 weeks.
Food Fortification
0035Although vitamin A supplementation is a simple and
effective intervention, it does not correct the under-
lying dietary causes. In recent years, food-based ap-
proaches have been receiving increasing attention as a
long-term sustainable strategy. Food fortification
offers a direct, effective, and potentially sustainable
way to correct VAD. Vitamin A fortification of sugar
has been successfully implemented in Guatemala and
other Central American countries. However, a recent
survey in Guatemala showed a high prevalence of
VAD in children < 3 years, suggesting that fortification
of a single food may not ensure adequate vitamin A
status of the entire population. Fortification of mul-
tiple foods, including complementary foods targeted
to young children, has been suggested as an alternate
strategy. Other foods fortified with vitamin A include
margarine in the Philippines, monosodium glutamate
in Indonesia, and edible oils in India. Selection of
appropriate vehicle and adequate level of fortification
are important to meet the population needs.
0036Since VAD often coexists with deficiencies of other
micronutrients like iron, folate, and zinc, fortification
of foods with multiple nutrients has been suggested.
Further research is needed to understand the inter-
actions of various nutrients and to establish whether
fortification with multiple nutrients would facilitate
each other’s beneficial effects.
3218 HYPOVITAMINOSIS A