Kallen A. Understanding Biostatistics
Подождите немного. Документ загружается.

48 OBSERVATIONAL STUDIES AND THE NEED FOR CLINICAL TRIALS
epidemiologists therefore choose other measures, including the Mantel–Haenszel pooled odds
ratio, which we will discuss later. The same is true of relative risks; geometrically it is a
consequence of the ratio of ratios situation discussed in Box 2.8.
Another point of confusion about confounders and the subgroups they define is called
stage migration. It originally referred to what appeared to be a paradox when one looked
into cancer survival by disease stage. Cancer stage is an indicator of a tumor’s anatomic
dissemination and is a key predictor of cancer survival. In its simplest form, a tumor may be
classified as ‘localized’ (Stage I) if there is no evidence of spread of the tumor beyond where
it originated, ‘regional’ (Stage II) if there is evidence of tumor spread to adjacent tissues or
lymph nodes but no further, and ‘metastatic’ (Stage III) if there is evidence that the tumor has
spread to other organs. The lower the stage, the better the prognosis. The apparent paradox
is that you may find, when you compare two studies, that they demonstrate the same overall
survival, but that in one study all the individual stages have improved survival compared to
the other study. This looks like a paradox, because you expect the sum to increase when all
the terms in the sum is increased.
Again this is not a paradox if properly expressed. A good insight is often attributed to
the US humorist Will Rogers in the following quotation: ‘When the Okies left Oklahoma
and moved to California, they raised the average intelligence level in both states.’ Put in a
medical context, assume that you use some test and divide a population into those that are
healthy and those that are sick. The former group has on average a longer expected survival
than the latter. Next assume that a new diagnostic tool is introduced which identifies some
of those formerly believed to be healthy to be sick. With this new classification the group of
healthy will have a longer expected survival than before, since that group has lost some of
its more fragile individuals. Also the group of sick will have an increased expected survival
time, since it has been augmented by a few almost healthy individuals. No individual has
changed expected survival, so the total average stays the same. The important point is that if
we compare the group of sick individuals in the two classifications, we would infer that now,
after the introduction of the new diagnostic tool, they have a longer survival. It is not a faulty
conclusion per se, but the survival has not changed for any individual.
A well-known conundrum related to stage migration is the so-called low-birthweight
paradox, which is discussed in some detail in the next example. It refers to the fact that data
tell us that a baby with low birthweight has a greater chance of being alive if the mother is a
smoker, which seems to imply that maternal smoking benefits the baby.
Example 2.3 The following table shows the relation between infant mortality and maternal
smoking in a region of Sweden in a particular year:
Mother
Infant Non-smoker Smoker
Stillborn 40 6
Liveborn 10 665 1 277
P(Dead) (%) 0.374 0.468
As we have learnt to expect, this shows that a smoking mother has an increased risk of having
a stillborn baby. The number of stillborns is small, so the precision in this data is not that

CONFOUNDERS, SIMPSON’S PARADOX AND STRATIFICATION 49
great, but it is consistent with data from many sources and parts of the world. However,
if we look only at children weighing less than 2.5 kg at birth, we seem to get a different
message.
Mother
Infant Non-smoker Smoker
Stillborn 19 1
Liveborn 371 73
P(Dead) (%) 4.87 1.35
Now the proportion of stillborn babies is larger for non-smoking mothers. Somehow it seems
that a low-birthweight baby increases its survival chance by having a smoking mother. Does
this mean that maternal smoking protects children with low birthweight?
There is no argument that the last table tells us that if we randomly choose a newborn with
a low birthweight (less than 2.5 kg), then the probability that it is alive is larger if the mother is
a smoker than if not. It is the conclusion from this observation that the mother’s smoking habit
has a beneficial effect on the babies survival chances that is wrong. This paradox is essentially
only another example of stage migration. The underlying reason is that maternal smoking
has a negative effect on the baby’s birthweight. The staging is the dichotomy into low and
high birthweight, where smoking means that we move some of the high-birthweight babies
into the low-birthweight group, carrying with them their original risk of being stillborn.
So we dilute the risk of death in the low-birthweight group by putting more ‘healthy’
babies there.
For the mathematically more interested reader we can build a model which captures a few,
but key, aspects of the situation.
•
Denote the distribution of the birthweight for babies of non-smoking women by F (x).
Also assume that smoking shifts this distribution to the left, so that the corresponding
distribution for smoking women is F (x + ) for some . (Our data estimate to be
199 grams.)
•
Assume that the weight distribution for stillborn babies is the same for smoking and
non-smoking mothers.
To what extent the second point holds true is not important to us, because we want to de-
scribe the effect of the first point, which we know is true, on the subgroup analysis made
above.
For illustration we will use Gaussian approximations to all distributions; these CDFs are
shown in Figure 2.3(a). Using the model above, we can construct subgroup tables similar to
the one above but for a general cut-off point x instead of the special case x = 2 .5 kg only. Let
W denote the birthweight and D denote the event that the baby is stillborn. Within one of the
groups of mothers, the fraction of stillborn babies among those with a birthweight at most x is
given by
P(D|W ≤ x) =
P(D and W ≤ x)
P(W ≤ x)
=
P(W ≤ x|D)P(D)
P(W ≤ x)
,
50 OBSERVATIONAL STUDIES AND THE NEED FOR CLINICAL TRIALS
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
Proportion of babies
4000300020001000
Birth weight (g)
N
o
n
-
s
m
o
k
i
n
g
m
o
t
h
e
r
s
S
m
o
k
i
n
g
m
o
t
h
e
r
s
S
t
i
l
l
b
o
r
n
b
a
b
i
e
s
(a)
0
0.1
0.2
Probability for a stillborn baby
300025002000
Birth weight (g)
N
o
n
-
s
m
o
k
i
n
g
m
o
t
h
e
r
s
S
m
o
k
i
n
g
m
o
t
h
e
r
s
(b)
0
0.3
0.6
0.9
1.2
Relative Risk
400030002000
Birth weight (g)
(c)
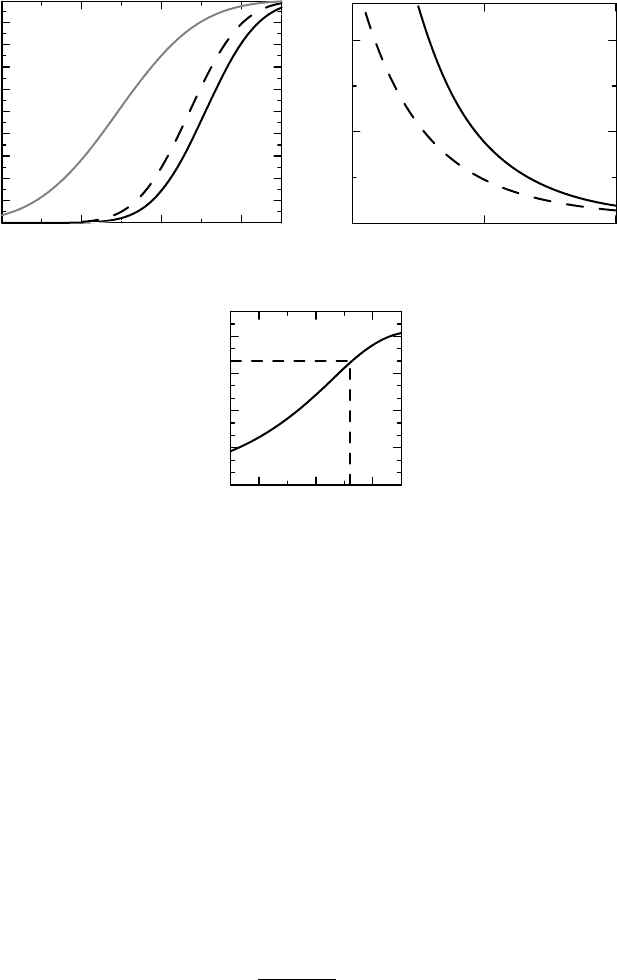
Figure 2.3 A model for the low-birthweight paradox. (a) The assumed birthweight distri-
butions for smoking and non-smoking mothers as well as the birthweight distribution for
stillborn babies. (b) The derived probability for a stillborn baby given an upper limit for the
baby’s weight, by the mother’s smoking status. (c) The relative risk for a stillborn child given
different cut-offs for baby weights. Further details in the text.
where P(W ≤ x|D) is assumed independent of group (the gray curve in Figure 2.3(a)),
P(D) is the overall probability of a stillborn baby and the denominator P(W ≤ x)isthe
distribution described in the first point above. This probability, as a function of the cut-off
point x, is plotted for the two groups of mothers in Figure 2.3(b). (The numbers do not quite
fit with the original subgroup table because of our simplifying assumption.) We see that
this probability is smaller for smoking mothers than for non-smoking mothers, irrespective
of which cut-off limit we choose. There is nothing special about the particular cut-off
limit of 2.5 kg. The relative risk for a stillborn baby for smokers versus non-smokers is
given by
RR(x) =
F (x)
F (x + )
RR(∞),
where RR(∞) = 1.23 > 1 is the overall relative risk. The graph of this function is plotted in
Figure 2.3(c). We see that it decreases as we decrease the cut-off point, which means that the
smaller we make it, the stronger the ‘paradox’. It only becomes favorable for non-smokers
if we take the cut-off at about 3.6 kg.
ON INCIDENCE AND PREVALENCE IN EPIDEMIOLOGY 51
2.7 On incidence and prevalence in epidemiology
There is often confusion about what is meant by the rate at which an event occurs and the
probability that it occurs. In fact, the two words are too often used interchangeably. This is not
a good habit, since rate is like speed, something that happens per time unit. Loosely speaking,
the rate at which an event occurs is an entity such that if we multiply it by some short time
interval in which the rate is essentially constant, we (approximately) get the probability that
the event occurs in that particular interval. If the event is adverse to the individual experiencing
it, the rate is often called the hazard for the event. Another term that is often used is intensity.
Obviously there is a relationship between the rate at which events occur, and the probability
that a randomly selected individual has experienced the event when observed. To model
this situation we assume that there is a constant intensity λ with which the event occurs.
Let Q(t) denote the fraction of subjects that have not experienced the event at time t. This
fraction decreases at a rate which is proportional to itself, which we mathematically write
as a differential equation Q
(t) =−λQ(t). (This is actually the definition of the intensity λ.)
Solving the equation, we find (since Q(0) = 1) that Q(t) = e
−λt
, so that the probability that
the event has occurred in the interval (0,T)isgivenby
p = 1 − Q(T ) = 1 − e
−λT
.
This is the relation between the rate of occurrence λ and the probability of the event occurring
during an observation time T .
H
I
D
α
μ
ν
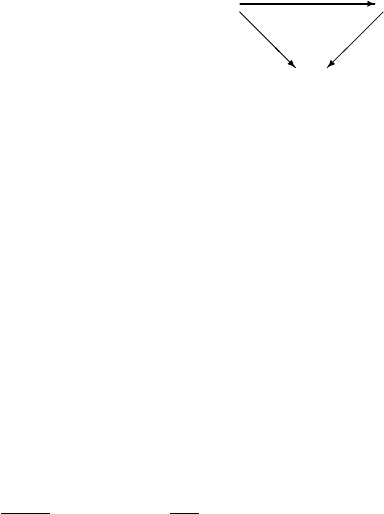
There are two important concepts in epidemiology which
are related to this discussion, the disease prevalence and the
disease incidence. The typical situation is described in the
diagram on the right, where H refers to the healthy individuals
in the population, D denotes death and I is the population with
the disease. The rate α is the disease incidence (for a healthy individual) and μ and ν are the
death rates for healthy and sick individuals, respectively. This diagram corresponds to two
differential equations, each built from the observation that the rate of change of individuals
in the population is the net effect of influx (the rate at which new people enter the population)
and outflux (the rate at which people are removed from that population). A healthy individual
can either get the disease or die without having contracted it, whereas a person with the
disease must have been healthy once, and is assumed to leave this disease state only by dying.
We assume that the disease is chronic, and the discussion is therefore not relevant for most
infectious diseases. Mathematically this is formulated as the two differential equations
H
(t) = β − (α + μ)H(t),I
(t) = αH(t) − νI(t),
where β represents a constant birth (or influx) rate. When this population is in equilibrium, the
left-hand sides of the two equations are zero, which gives us the two steady-state populations
¯
H =
β
α + μ
, and
¯
I =
α
¯
H
ν
.

52 OBSERVATIONAL STUDIES AND THE NEED FOR CLINICAL TRIALS
The factor ν
−1
is the (mean) duration of the disease (until death). The prevalence P of the
disease is the fraction of subjects that have the disease:
P =
¯
I
¯
I +
¯
H
=
α
α + ν
,
which is a proportion. The corresponding odds is given by
P
1 − P
=
α
ν
= incidence × duration.
In particular, this means that if we have two groups of patients and compute the prevalence
odds ratio, this is the ratio of the incidences multiplied by the ratio of the durations in the two
groups. If we further assume that the duration of the disease is the same in the two groups, the
prevalence odds ratio equals the ratio of the disease incidences for the two groups. We must
keep in mind that these are statements about populations that are in steady state.
The incidence α is the number of cases per unit time. To estimate it, we start with the
following equation for the healthy group:
H
(t) =−(α + μ)H (t),H(0) = H
0
,
which has the solution H(t) = H
0
e
−(α+μ)t
. If we count only new cases, N(t), these increase
during the observation period at a rate that is proportional to the size of the healthy population.
This means that N
(t) = αH(t), from which it follows that
N(t) =
αH
0
α + μ
(1 − e
−(α+μ)t
), 0 <t<T.
If we ignore the deaths here and take μ = 0, we have that the cumulative incidence function
(CIF) G(t) = N(t)/H
0
of new cases is given by G(t) = 1 − e
−αt
. This quantity is (approx-
imately) what we observe, and from it we can obtain the estimate for α.Ifα is small, we
have G(t) ≈ αt, so we estimate α as the observed number per person-year. Better than to
ignore deaths is to consider such events as censored; an individual who dies without having
developed the disease can only be counted as being at risk before he dies. This means that we
observe this individual for only a part of the observation period, which we should take into
account when we estimate α. This is further discussed in Chapter 11.
The CIF gives the proportion of individuals observed for whom the event has occurred
at a particular point in time. A related question is this: what is the distribution of the total
number of events that occur – for example, the number of subjects who will acquire the disease
in the population we study during the observation time? The discussion in Box 2.10 shows
that it is a reasonable approximation when the events are rare enough (so that there is not
much difference between the conditional mean hazard and the overall mean hazard) that this
number has a Po(αT ) distribution, where T is the total exposure time for the whole group
and α is as above. There is an implicit assumption here that the disease is not contagious,
since that would make events come in clusters, which we assume is not the case. (Note that
the Poisson approximation implies that α is estimated by the number of events divided by
observed person-years.)
COMMENTS AND FURTHER READING 53
Box 2.10 The Poisson distribution and Poisson process
Consider a large population in which a particular disease occurs with a subject-specific
but constant hazard rate, which therefore defines a stochastic variable θ. Assume also
that the events are rare in the population. If we start a clock and count the cumulative
number N(t) of disease occurrences up to time t in the population, we get a stochastic
variable which, to a good approximation, has a Poisson distribution. Here is a heuristic
explanation.
Let P
k
(t) = P(N(t) = k) be the probability that exactly k events have occurred
before time t and assume that events do not come in clusters. We then have for s>t
but very close to t that (approximately, but with an error which we ignore)
P
k
(s) = P(N(s) = k|N(t) = k)P
k
(t) + P (N(s) = k|N(t) = k − 1)P
k−1
(t).
If we differentiate this with respect to s and then let s → t, we find that
P
k
(t) =−λ(t)P
k
(t) + λ(t)P
k−1
(t),k > 0,P
0
(t) =−λ(t)P
0
(t),
where λ(t) = E(θ|T ≥ t) is the average hazard rate among those who have not yet had
an event at time t. The general solution to this system of differential equations is
P
k
(t) =
(t)
k
k!
e
−(t)
, where (t) =
t
0
λ(s)ds
is the cumulative intensity function in the population. This means that N(t) ∈ Po((t)),
where Po(μ) denotes the Poisson distribution with mean μ. This is the discrete distri-
bution that takes on the values k = 0, 1,...with probabilities e
−μ
μ
k
/k!. The Poisson
distribution is one of the important distributions in elementary statistics. One of its
more important properties is the addition formula that if X is distributed as Po(μ
1
)
and Y as Po(μ
2
), then X + Y is distributed as Po(μ
1
+ μ
2
), provided the variables
are independent.
2.8 Comments and further reading
Much of the early discussion in this chapter is about epidemiology and case–control studies,
to which Rothman (2002) may serve as an introduction. The style of the beginning of this
chapter was much inspired by the book by Evans et al. (2006), which is now (as of this
writing) out of print, but can be found on the Internet in the James Lind Library, a site
devoted to explaining and illustrating the development of fair tests of treatment in health
care. The particular epidemiological story about lung cancer and smoking is discussed by
Richard Doll (1998b) in a volume of Statistical Methods in Medical Research which has the
statistics of smoking as its theme; the quote from Thomas Lewis at the end of Section 2.2) is
taken from Doll (1998a). The original articles referred to in Box 2.3 are Doll and Hill (1950,
1956). The causality question here is interesting in itself, since some eminent statisticians,
R.A. Fisher in the UK and Berkson in the US, remained unconvinced about the interpretation
that this was evidence for smoking as a causative factor. (For Fisher the argument seems to
54 OBSERVATIONAL STUDIES AND THE NEED FOR CLINICAL TRIALS
have been around a common genetic cause for both lung cancer and the smoking habit, or
one preventing both.) However, biology has moved on since then, and now the importance
of smoking in the development of lung cancer is beyond any reasonable doubt, despite the
non-existence of a properly randomized trial to confirm this. In addition to this there are
numerous other diseases for which there is clear evidence that smoking is an important risk
factor, including cardiovascular disease. The WHI study reference mentioned in Box 2.4 is
Writing Group for the Women’s Health Initiative Investigators (2002).
The importance of James Lind in combating scurvy is debated in (Wootton, 2007, Chap-
ter 8), where it is argued that the importance of this particular experiment is a modern con-
struction with no support in history. Lind had no influence on subsequent developments, and
perhaps did not understand what he had discovered himself. In the same book, Chapter 16 also
contains a discussion about what happened after the 1950 result of Doll and Hill on smoking
and lung cancer.
We noted above that the odds ratio may be the preferred way to describe an association
ina2× 2 table, because it is independent of the study design. The main argument against its
use is that the odds ratio is hard to interpret, but there is also an argument that the strength of
an association should not be measured in this way at all. A critique of the odds ratio, together
with a general discussion about different measures that can be obtained from the four numbers
ofa2× 2 table, is given by Kraemer (2004).
Simpson’s paradox was extensively studied in Simpson (1951), but had been observed
and discussed earlier. An in-depth discussion of it, and the causality problem, is given
by Pearl (2000). Cornfield’s inequality (Cornfield et al., 1959) appeared as a response to
Fisher’s suggestion of a common genetic cause for smoking and lung cancer. The kidney
stone example is taken from Charig et al. (1986) and has been used by others to this end. The
low-birthweight paradox is discussed in Wilcox (2001), where it is shown that our quantitative
argument applies better as a high-altitude paradox than a low-birthweight paradox. This paper
demonstrates that life at high altitudes (as in Norway or Colorado, US) leads to a shift in the
birthweight distribution in the same way as maternal smoking does, but has no effect on child
mortality. When it comes to smoking, it turns out, not surprisingly, that smoking actually has
an effect on mortality – it increases it. In other words, the true effect is the reverse of what the
paradox claim.
The discussion in the last section was focused on the relationship between the two concepts
incidence and prevalence in epidemiology, but is also the starting point for some statistical
models with important application in biostatistics. What we have is a competing risk model,
where the acquiring of the disease is in competition with death without having acquired it.
This type of model will be revisited in Chapter 11.
References
Charig, C., Webb, D., Payne, S. and Wickham, O. (1986) Comparison of treatment of renal calculi by
operative surgery, percutaneous nephrolithotomy, and extracorporeal shock wave lithotripsy. British
Medical Journal, 292, 879–882.
Cornfield, J., Haenszel, W., Hammond, E., Lilienfeld, A., Shimkin, M. and Wynder, E. (1959) Smoking
and lung cancer: Recent evidence and a discussion of some questions. Journal of the National Cancer
Institute, 22, 173–203.
Doll, R. (1998a) Controlled trials: the 1948 watershed. British Medical Journal, 317, 1217–1220.
REFERENCES 55
Doll, R. (1998b) Uncovering the effects of smoking: historical perspective. Statistical Methods in Med-
ical Research, 7(2), 87–117.
Doll, R. and Hill, A.B. (1950) Smoking and carcinoma of the lung. preliminary report. British Journal
of Medicine, 2(4682), 739–748.
Doll, R. and Hill, A.B. (1956) Lung cancer and other causes of death in relation to smoking; a second
report on the mortality of British doctors. British Journal of Medicine, 2(5001), 1071–1081.
Evans, I., Thornton, H. and Chalmers, I. (2006) Testing Treatments. Better research for better healthcare.
London: British Library.
Kraemer, H.C. (2004) Reconsidering the odds ratio as a measure of 2 × 2 association in a population.
Statistics in Medicine, 23, 257–270.
Pearl, J. (2000) Causality: Models, Reasoning, and Inference. Cambridge: Cambridge University Press.
Rothman, K.J. (2002) Epidemiology. An introduction. Oxford: Oxford University Press.
Simpson, E. (1951) The interpretation of interaction in contingency tables. Journal of the Royal Statis-
tical Society, Series B, 13, 238–241.
Wilcox, A.J. (2001) On the importance – and the unimportance – of birthweight. International Journal
of Epidemiology, 30, 1233–1241.
Wootton, D. (2007) Bad Medicine: Doctors Doing Harm since Hippocrates. Oxford: Oxford University
Press.
Writing Group for the Women’s Health Initiative Investigators (2002) Risks and benefits of estrogen plus
progestin in healthy postmenopausal women. principal results from the Women’s Health Initiative
Randomized Controlled Trial. Journal of the American Medical Association, 288(3), 321–333.

3
Study design and the bias issue
3.1 Introduction
In our first chapter we discussed the different steps that are involved when evidence is obtained
using statistical methods. Not only do we need the experiment to provide us with the data for
analysis, we also must ensure that the design allows us to draw the conclusions we want to from
this statistical analysis. A small p-value alone does not guarantee the validity of the conclusion.
The design elements that were discussed included the importance of avoiding the multiplicity
issue. This has become a statistical issue, because of the habit of forcing conclusions from
p-values. However, even when we have planned our statistical work properly, and know how
to draw conclusions from such information, there remain design problems to be addressed.
These are not really statistical issues, but are very often considered to be so by physicians
when it comes to medical research. They are about eliminating alternative explanations from
the experiment.
In the previous chapter we discussed clinical study design in terms of what kind of studies
we can do. Here we will discuss in more detail some aspects that relate to the problem of how
to avoid bias. Bias is about having some alternative explanation operating in the background
which influences the result, but which is not acknowledged when the conclusions are drawn.
Understanding the bias problem has led to the development of the controlled, randomized,
double-blind, clinical study as the state-of-the-art study design when it comes to clinical
research, provided it can be done. We will address different aspects of bias, pointing out what
it is randomization and blinding try to accomplish. Following that we will take a look at the
analysis stage. Statisticians, especially in the pharmaceutical industry, have invented ways to
undo some of the careful planning that goes into a state-of-the-art clinical study. I call this
self-inflicted bias, where the generally accepted term is that a per protocol (PP) analysis is
done. It is about selecting data for analysis, and we will see an example which shows how
data, which are originally unbiased, become biased despite the best of intentions.
In Section 3.9 we will address the bias involved when we try to obtain knowledge by
summarizing the medical literature. Decisions taken from such reviews are what is generally
referred to as evidence-based medicine. This involves combining results from different studies
Understanding Biostatistics, First Edition. Anders K¨all´en.
© 2011 John Wiley & Sons, Ltd. Published 2011 by John Wiley & Sons, Ltd. ISBN: 978-0-470-66636-4
58 STUDY DESIGN AND THE BIAS ISSUE
reported in the literature in so-called meta-analysis. The bias referred to is the publication
bias which follows from the fact that it is predominantly positive findings that get published.
3.2 What bias is all about
In everyday language bias is about prejudice – about opinions or feelings that tend to favor
one side in an argument. In statistics in particular, and science in general, it is any factor or
process that tends to drag the results away from the truth. To clarify what this means in a
statistical context, consider a situation where we have compared two groups.
•
The statistical methodology, including the p-value, tells us what confidence we can
have that there is a difference between the groups for the outcome measure we have
analyzed.
•
Our objective is usually not to claim that there is a difference between the groups but
to claim that the difference is due to a particular factor, such as a drug treatment, which
defines the groups. The question is whether this is a valid conclusion to draw from the
statistical analysis.
Bias enters at both these stages; in the first stage because many statistical methods have some
intrinsic, but usually rather mild, bias built into the estimation of the effect. In this chapter we
ignore this particular kind of bias and concentrate fully on the issue in the second stage: how
we certify that we are making the right claim.
The basic point which we must bear in mind at all times is this: if we want to prove that
a particular exposure increases the risk of an outcome Y , or the magnitude of an outcome
variable Y , we may divide patients into two groups, exposed and non-exposed, and analyze
how Y differs between the two groups. The confidence in the conclusion about Y hinges on
the extent to which we can guarantee that the two groups do not differ in any other respects
than the exposure factor. When we say ‘differ’, we are not referring to the random differences
that always will occur when you sample from two groups, and which are handled by the
statistical methodology. What we are referring to are any systematic differences, which is what
defines bias.
In coming sections we will discuss the following basic variants of bias:
•
selection bias, which occurs when our sample is not representative of the population we
want to make claims about;
•
incomparable groups (apart from the factor(s) under investigation) when we start, and
how we use randomization in experimental studies to avoid this;
•
information bias, which refers to when the measurements are not taken in identical ways
in the two groups – this includes differences in the conduct of the study in the groups
of an intervention study.
3.3 The need for a representative sample: on selection bias
The simplest example of bias is when our purpose is to obtain a description of a population,
using a sample from it. It could be something as simple as the male/female ratio in the