Marshall L. Stoller, Maxwell V. Meng-Urinary Stone Disease
Подождите немного. Документ загружается.

380 Breiman and Coakley
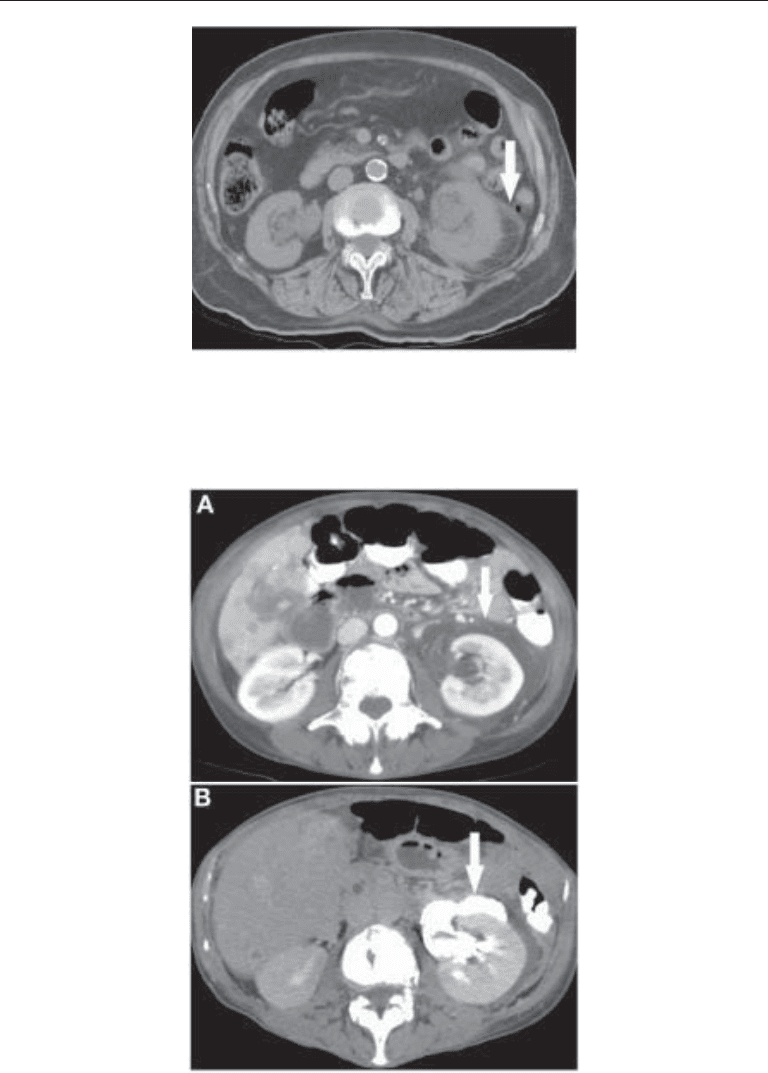
Fig. 11. Perinephric fat stranding (arrow) around the left kidney caused by a distal obstructing
stone (not shown). Perinephric fat stranding in this setting reflects edema and distended lymphat-
ics, and is often associated with a loss of definition of renal contours.
Fig. 12. (A) Contrast enhanced CT in a patient with metastatic breast cancer and acute left sided
flank pain. Images at a lower level (not shown) showed a 5 mm stone in the left ureterovesical
junction. Note the presence of fluid (arrow) around the left kidney. (B) CT image obtained 15
mins later. Excreted contrast is seen to pass from the left pelvicaliceal system into the left
perirenal space (arrow), confirming the diagnosis of forniceal rupture secondary to calculous
obstruction.

Chapter 20 / Imaging of Urinary Stone Disease 381
peristalsis, with a potential paradoxical decrease in pain. Complete obstruction lasting
4–7 d or partially for 14 d may result in various degrees of irreversible decrease in renal
function (24,25).
SPECIFIC IMAGING MODALITIES IN URINARY STONE DISEASE
Overview: Imaging Evaluation of Acute Flank Pain
The primary diagnostic consideration in a patient with acute flank pain is an obstruct-
ing ureteral stone. Consequently, studies investigating imaging algorithms typically use
identification of a ureteral stone as the end-point. This obscures the fact that the radio-
logical evaluation of acute flank pain should answer two related but distinct questions—
is urinary obstruction present and, if so, what is the level and cause of obstruction? The
presence or absence of ureteral obstruction is a functional question, whereas cause and
level are anatomic issues. Many imaging tests are primarily anatomic or functional in
nature. The apparently conflicting views on appropriate imaging in acute flank pain
often reflect a conceptual failure to distinguish these two issues. US and noncontrast
enhanced CT (NCCT) use the anatomic findings of hydronephrosis and hydroureter as
indirect indicators of obstruction, but do not provide direct functional assessment.
Only contrast-enhanced CT and IVU provide direct functional information. Plain radio-
graphs provide no meaningful evaluation of obstruction, but can directly demonstrate
the cause and level of obstruction, if obstruction is a result of a radiographically demon-
strable calculus. US rarely directly visualizes the cause of obstruction. CT can depict the
cause and level of obstruction in nearly all cases.
Plain Radiography
In the past the first imaging study requested in patients with acute flank pain was
frequently a plain radiograph (also known as a conventional abdominal film, abdominal
flat plate, or KUB; the latter refers to inclusion of the kidneys, ureters, and bladder in the
field of view). Detectability of stones on conventional radiographs depends on size and
composition as well as factors relating to technique, patient body habitus and overlying
structures, such as bowel contents. In theory 90–95% of stones are sufficiently radio-
paque to be visible by plain radiography (26). In practice, the plain radiograph is limited
in the evaluation of renal colic because multiple radiodensities can mimic stones (e.g.,
gallstones, costochondral calcifications, bone islands, and fecal densities) and stones
may be easily missed (e.g., radiolucent stones, and stones obscured by bowel content or
bone) (Fig. 13). Bowel preparation has been traditionally thought to improve detection
of stones, but a recent randomized study failed to confirm this hypothesis (27). These
limitations are illustrated by the reported accuracy of plain radiographs for renal colic.
In a study of 51 patients, using IVU as the gold standard, the sensitivity was 29% and
specificity was 73% (28). In a study of 49 patients, using stone passage or retrieval as
the gold standard, plain radiography had a sensitivity of 68% and a specificity of 96%
(29). In another study of 40 patients, using stone passage or retrieval as the gold standard,
plain radiography had a sensitivity of 54% and a specificity of 67% (30). The sensitivity
of a plain radiograph for the detection of urinary calculi ranges from 45 to 58% when
NCCT is used as the standard (31–36). The addition of nephrotomography improves
radiographic sensitivity by 30–40%, but patient radiation dosage is increased signifi-
cantly and overall accuracy remains well below NCCT (35). Plain radiographs remain
useful in the planning and the guidance of shock-wave lithotripsy (SWL) and in moni-
382 Breiman and Coakley
toring the progress of a stone treated conservatively or stone fragments after lithotripsy,
provided the stone can be seen on plain radiographs and has been confirmed by CT.
In some centers, digital radiographs (DR) or computed radiographs (CR), and scanned
projection radiographs (SPR), including CT scout radiographs, serve as an alternative to
conventional film screen-based radiographs for stone detection and follow-up. The scout
radiograph, obtained at the time of a diagnostic CT, may be used as a baseline study in
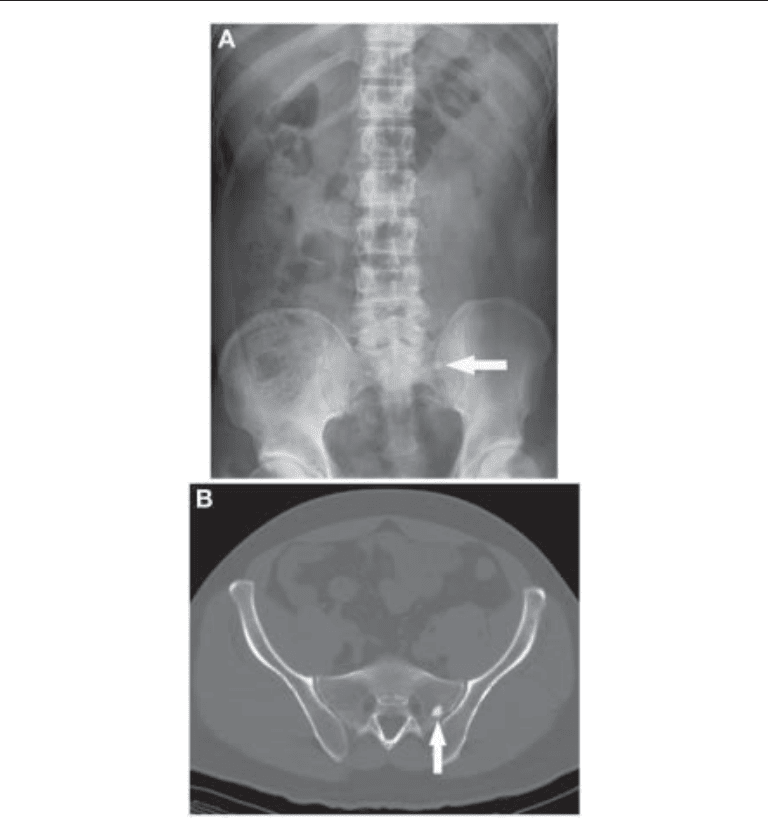
Fig. 13. (A) Plain abdominal radiograph in a patient with left flank pain. A small calcific density
(arrow) is seen projected over the left sacroiliac joint, and was initially interpreted as suggestive
of a ureteral calculus. (B) Axial CT image (shown at bone windows) through the level of the
density seen in (A) shows that the appearance is caused by a bone island (arrow) in the left side
of the sacrum. This example illustrates the known limitations of plain radiography in the assess-
ment of flank pain, because there are multiple causes of both false positive and false negative
results.

Chapter 20 / Imaging of Urinary Stone Disease 383
those patients to be followed with plain radiographs and may help in predicting the
success of radiographs for monitoring the progress of stone passage and whether stone
opacity is adequate to allow radiographic or fluoroscopic guidance of lithotripsy plan-
ning (32). Digital scout radiographs may also help predict stone composition, as a large
stone seen on CT but not evident on the scout view likely contains little calcium and a
high concentration of uric acid or xanthine (32). The resolution of digital radiographs is
slightly less than that of conventional radiography. Averch (37) showed the accuracy of
these modalities to be similar for detection of stones, whereas Assi (31) demonstrated
a significantly lower sensitivity of the scout radiograph compared with conventional
radiography, particularly for stones 3 mm or less in diameter.
Intravenous Urography
Until the advent of spiral CT, the excretory or intravenous pyelogram or IVU was the
gold standard for the evaluation of urolithiasis for over 70 yr (Fig. 14). It is a relatively
safe and accurate means of diagnosing and characterizing urinary calculi, yielding infor-
mation on renal function as well as anatomy. The IVU is particularly useful in document-
ing complex or subtle abnormalities of the urinary tract that may lead to stone formation
or complicate management. Nonopaque radiolucent stones can be detected as filling
defects within the collecting system, ureters or bladder. An IVU can usually differentiate
renal calcifications and calculi from extrarenal calcifications but may not always be able
to differentiate renal parenchymal calcifications from calculi. The location and size of
a calculus, the precise relationship of a renal calculus to the renal collecting system, and
the degree of resultant obstruction can be assessed with an IVU. Underlying anatomic
abnormalities predisposing to stone formation, or affecting the choice of therapy, can be
assessed as well. A logistical disadvantage of IVU is that a physician must be present
because of the risk of contrast reactions. This may limit the availability of IVU in small
departments with fewer personnel or off-site coverage. Another disadvantage is that the
study may be protracted in patients with obstruction, when delayed images may be
required several hours after injection of contrast for complete assessment. The emer-
gence of NCCT as the primary test in patients with flank pain also exposes physicians
who still request or perform IVU for this indication to medicolegal liability in the event
of a contrast reaction. In a case where an emergency IVU resulted in a fatal contrast
reaction, the subsequent settlement distributed 90% of the responsibility to the perform-
ing radiologist and 10% to the ordering urologist, despite an attempt by the radiologist
to convince the urologist that a noncontrast CT had become the community standard.
Criminal manslaughter charges were also pressed, but were eventually dropped (38).
Although the IVU for flank pain is rapidly passing into history, the imaging findings
of urolithiasis on IVU remain of interest. Following calculous ureteral obstruction, the
nephrogram may initially be normal, but later becomes dense and associated with
delayed excretion as tubular filtration decreases (Fig. 14). Fine striations related to
dilated tubules may be present in the area of the renal pyramids. Opacification of the
obstructed collecting system may take as long as 24 h when the obstruction is severe.
As excreted contrast is heavier than unopacified urine, a change in patient position may
be helpful in opacifying previously unopacified portions of the collecting systems or
ureters. Radiolucent stones may be identified as filling defects on an IVU (Fig. 4). If
a stone is similar in density to excreted contrast, it may not be recognized on excretory
films, and may be only visible on the precontrast scout radiograph. An IVU may be
helpful in differentiating intra- from extraluminal opacities. A stone impacted at the
384 Breiman and Coakley
ureterovesical junction may create an apparent bladder wall mass on an IVU. This
pseudomass is most frequently associated with stones lodged in the ureterovesical
junction. Edema surrounding an impacted UVJ stone may create a pseudoureterocele.
Nodular bladder wall edema may simulate a bladder neoplasm. Overall, although IVU
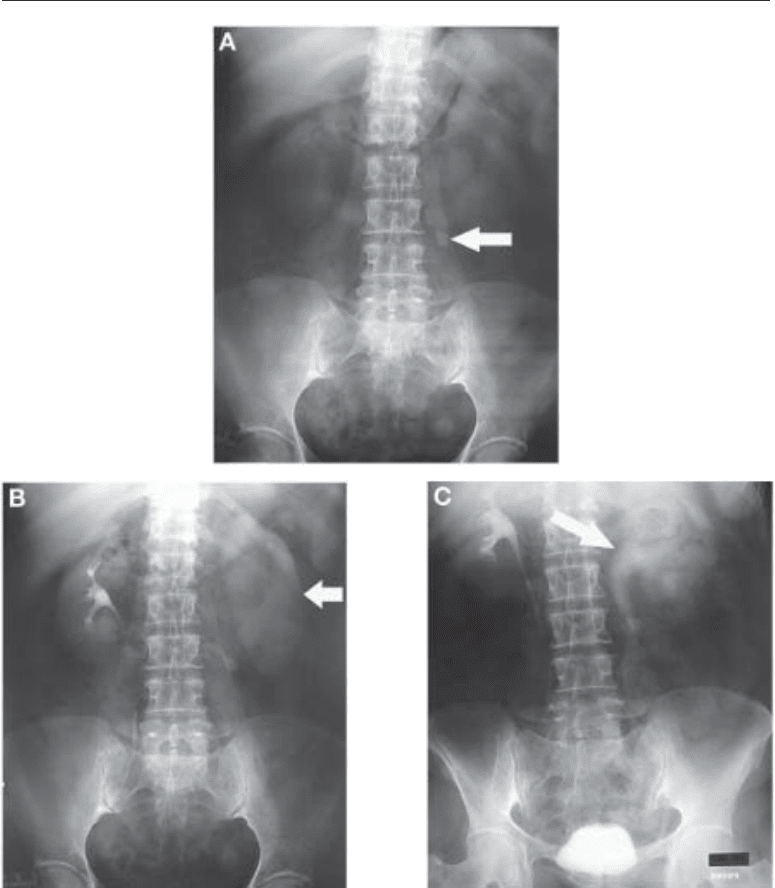
Fig. 14. (A) Scout radiograph from an IVP shows a 2 cm calcific density (arrow) at the left L3/
4 disc space. (B) Five-minute film shows asymmetry of the upper tracts. The right nephrogram
and pelvicaliceal system are unremarkable, whereas the left kidney is enlarged with a dense
nephrogram and delayed excretion. These findings are typical of obstruction. (C) Thirty-minute
film shows contrast excretion into a dilated left pelvicaliceal system (arrow) and ureter, to a level
of the previously noted calcific density. The findings confirm the diagnosis of an obstructing
ureteral calculus.

Chapter 20 / Imaging of Urinary Stone Disease 385
reliably demonstrates obstruction, the cause is not always clearly delineated. In a series
of 46 patients with calculous ureteral obstruction, the stone was not visible at IVP in 6
(13%) (39). The six missed stones were confirmed by retrograde pyelography, ureter-
oscopy, or spontaneous passage. In two other series, obstructing stones were missed by
IVU in 12 of 28 and 6 of 11 patients (30,40). The emergence of NCCT probably
accounts for the apparent drop in IVU sensitivity for stone identification. In the past,
an IVU showing mild hydroureteronephorosis but no stone was often reported as “pos-
sible recent stone passage.” It is possible that many of these cases were caused by small,
urographically occult stones.
Persistent urinary obstruction may result in forniceal rupture. The resultant decrease
in pressure from the forniceal rupture may result in symptomatic relief and be mistaken
for stone passage. A forniceal rupture of short duration and in the absence of infected
urine is usually of no clinical significance. Perinephric fluid resulting from a forniceal
rupture is important to differentiate from perinephric edema and fat stranding in a patient
with infected urine, however, as prophylactic antibiotic treatment may be administered
to avoid perinephric abscess formation. Other findings of acute ureteral obstruction
include an enlarged ipsilateral kidney (nephromegaly), and hydronephrosis or hydro-
ureter.
Intravenous iodinated contrast may be required for IVU or CT urography (CTU), so
a brief discussion of safety is warranted. Contrast reactions range from mild hives with
pruritis to bronchospasm, hypotension and anaphylactic reaction or death. Low osmo-
lality nonionic contrast agents, available since the late 1980s, have reduced the risk of
severe reactions by approx 80%. The risk of fatal anaphylaxis following intravenous
contrast is approx 0.9/100,000 with both high and low osmolality contrast (41). Premedi-
cation regimens including steroids and both histamine-1 and histamine-2 blockers re-
duce the risk of contrast reactions, but have not been shown to specifically reduce the risk
of death. Nephrotoxicity is the other major adverse effect of intravenous contrast. Strat-
egies to reduce the frequency of nephrotoxicity, particularly in high-risk patients such
as those with diabetes or renal impairment, include hydration, premedication with
acetylcystine, or use of iso-osmolar dimeric contrast media (41–43).
Ultrasound
US may be used to directly depict stones, to identify hydronephrosis in calculous
ureteral obstruction, or to guide therapy such as percutaneous nephrostomy tube place-
ment, SWL, and percutaneous nephrolithotomy. The advantages of US include safety
(no iodinated contrast or ionizing radiation), availability, and lower cost relative to
CT. The disadvantages are related to limited accuracy, and will be discussed in greater
detail.
Calculi reflect sound creating echogenic, bright foci with acoustic shadowing deep to
the calculus (Fig. 15). Calculi that have a high percentage of matrix rather than calcium
may be echogenic without acoustic shadowing. Small stones, less than 5 mm, may be
difficult for US to confidently diagnose, as they are less likely to cast an acoustic shadow.
The use of a higher frequency transducer, 5–10 MHz, increases the echogenicity of small
stones and accentuates shadowing, but is associated with decreased beam penetration,
which often limits its application particularly in medium sized to large patients. Renal
parenchymal calcifications and focal echogenic renal sinus fat may be difficult to dis-
tinguish from stones by US. The difficulty in depicting small echogenic stones against
a background of echogenic renal sinus fat should not be underestimated, and represents
386 Breiman and Coakley
a major limitation of sonography for diagnosis of renal calculi. In a recent study using
nonenhanced CT as the gold standard, US only detected 24 of 101 calculi, with a speci-
ficity of 90% (44).
US is used to identify obstruction by demonstration of hydronephrosis rather than by
direct visualization of a stone (although an obstructing calculus may sometimes be seen
high in the ureter through the acoustic window for the kidney, or in the distal ureter
through the bladder). Bowel and bone limit acoustic access to the rest of the ureter in
the retroperitoneum. The main drawback of US is that not all obstructed kidneys have
dilated pelvicaliceal systems, either because dilatation has not yet developed, the upper
tract has decompressed by forniceal rupture (45), or the upper tract is noncompliant. In
addition, the diuretic effect of intravenous contrast likely explains why dilatation is
occasionally absent at US but present at IVU (45). Reports of the false negative rates
for US include absence of dilation in (1) 8 of 21 (38%) patients with a delayed
nephrogram on IVU (29); (2) 7 of 20 (35%) patients with clinically proven obstruction
(45); (3) 3 of 53 (6%) patients with IVU-proven obstruction (39); and (4) 5 of 14 (36%)
patients with IVU-proven obstruction (46).
The false negative rate of 6–38% for US in acute renal colic represents a major
limitation. Doppler US has been advocated as a method of identifying nondilated
obstructed kidneys, based on the increased vascular resistance in obstructed kidneys.
However, this is not widely used because the results have been disappointing and the
technique is operator dependent (46). The addition of forced diuresis has been sug-
gested (47), but is not in common use. Color flow Doppler may be useful in assessing
ureteral jets in the bladder. On average, 1–12 jets of urine arising from the ureteral
orifices will be observed per minute in an asymptomatic patient (Fig. 16). Ureteral jets
are usually symmetric in appearance. Asymmetry of visible ureteral jets on color flow
Doppler or asymmetric flow velocity on pulsed Doppler may suggest ureteral obstruc-
tion on the side of reduced flow. For this sign to be most useful, the patient must be
well hydrated. As some nonobstructed patients demonstrate variability in the pattern
and symmetry of ureteral jets, this technique is felt to be of limited usefulness.
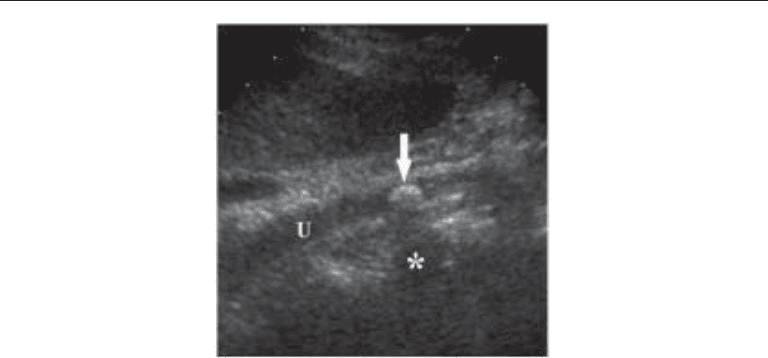
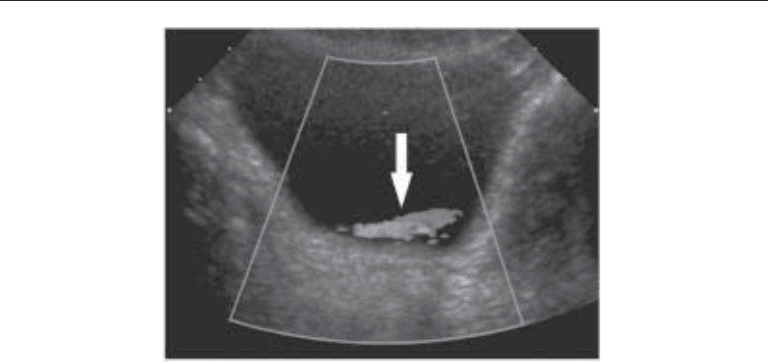
Fig. 15. Ultrasound image in a patient with right-sided flank pain. The right ureter (U) is dilated to
the level of an echogenic stone (arrow) that is casting a characteristic acoustic shadow (asterisk).
Chapter 20 / Imaging of Urinary Stone Disease 387
Combined Plain Radiography and Ultrasound
Given the limitations of KUB and US individually, there is no good reason to believe
that the combination is superior to either modality alone. This is generally supported by
the literature, with the exception of one paper that claimed that the combination was
100% sensitive and specific (100%), because all stones missed by US were fortuitously
visible on KUB (48). A more plausible study reported a sensitivity of 80% and a speci-
ficity of 58% for a combination of both tests (29).
Computed Tomography
Although many stones are radiolucent on plain radiographs, essentially all stones are
sufficiently dense to be visible on CT. The only exceptions are the urinary stone/sludge
formation associated with indinavir (49) and the very rare pure matrix stone composed
of mucous and debris (50). Therefore, the terms radiopaque and radiolucent are only
appropriate for plain radiography, and should not be used in the context of CT. The
volumetric capability of spiral CT allows rapid acquisition of overlapping thin slices
without the possibility of missing small stones between slices. The advent of spiral CT
has revolutionized the imaging of urinary stone disease, and noncontrast spiral CT has
emerged as a highly accurate modality for the identification of ureteral calculi. In a
comparative study of IVU and noncontrast CT in 40 patients with flank pain, 28 with
stones proven by retrieval or passage, IVU had a sensitivity and specificity of 64% and
92%, compared to 100% and 92% for noncontrast CT, respectively (30). Another study
of stone detection by noncontrast CT reported a sensitivity of 97% and a specificity of
96%(51). False positives and negatives are still possible because stones may be mistaken
for phleboliths or vascular calcifications, and vice versa. Contrast can be administered
in difficult cases to resolve any doubts. Other advantages of CT include better stone
characterization and anatomic localization, improved depiction of nonstone pathology,
and speed. CT allows examination of the entire abdomen and pelvis in a single breath
hold in most patients on modern multi-slice helical scanners. NCCT acquisition times
Fig. 16. Axial Doppler ultrasound image of the bladder demonstrating a right ureteral jet (arrow).
On average, 1–12 jets of urine arising from the ureteral orifices will be observed per minute in
a normal person.

388 Breiman and Coakley
are less than a minute and usually less than 20 s on multislice CT scanners, approx
10 s with 16 slice helical scanners. Because contrast is not required, NCCT is particularly
useful in patients with contrast allergy or impaired renal function. As intravenous iodi-
nated contrast is not administered, NCCT does not require a physician or nurse in atten-
dance during scanning, increasing the accessibility of the examination after hours. NCCT
for urinary stones has been criticized as lacking a functional component, as compared to
IVU, because contrast is not administered. This may limit the ability to depict obstruc-
tion based on an asymmetric nephrogram or delayed excretion. However, the assessment
of the chronicity and severity of obstruction may not significantly contribute to manage-
ment decisions or to the success of therapy. With respect to the radiation dose delivered
by CT, the risks of low dose radiation are controversial; there is general agreement that
the lowest reasonable dose that allows a diagnostic study should be used (52).
C
OMPUTED-TOMOGRAPHY TECHNIQUE
In our institution, we scan patients on single, 4, 8, and 16 slice helical scanners. We
select an mA in a range of 100–450, commensurate with the size of the patient, 240 mA
on average, with a higher mA selected for larger patients. Automatic modulation of mA
is available on some CT scanners. This modulates the mA on a scan-by-scan basis as
needed to achieve a preset level of image quality, accounting for the thickness and
X-ray attenuating characteristics of the tissues present in the area included in the slice
volume. The mA (and radiation dose) would be lower through the upper abdomen, which
include the lung bases (which attenuate relatively little X-ray), than through the pelvis,
which includes the iliac bones (which greatly attenuate X-rays), for example. Reduction
of mA helps lower radiation dose, without compromising stone detection (52). When
using a 16 slice scanner, we obtain 3 mm contiguous scans with the patient in the prone
position, with a pitch of 0.9, a rotation time of 0.75 s per rotation and 120 kVp. No
intravenous or oral contrast is initially administered. Patients are scanned prospectively
in the prone position to aid in distinguishing a bladder stone from a stone impacted in the
interureteric ridge portion of the ureterovesical junction, which may simulate a bladder
stone on a supine image (53) (Fig. 17). In our institution, noncontrast scans obtained to
search for urinary calculi are performed prospectively in the prone position, avoiding the
need to rescan with the associated reduction in radiation dose, prolongation of the exami-
nation, or need to recall the patient if the need for prone images was not recognized while
the patient was still in the department.
With multi-slice helical CT scanners, it is also possible to retrospectively create
thinner slices from the original standard thicker source images. Retrospective targeted
high-resolution reconstructions decreasing pixel size and increasing spatial resolution
may also supplement routine scans when needed (Fig. 18). These retrospective recon-
structions can be performed without the physical presence of the patient, as long as
source image raw data is still available. On newer scanners, raw data is usually available
for 12–36 h, depending on the number of patients scanned and the complexity of their
examinations. As mentioned previously, multiplanar reformations (MPR) may also be
helpful in resolving diagnostic dilemmas. MPRs and three-dimensional reformations
require only image data and not raw source data, allowing manipulation years after the
original examination, presuming digital data has been archived.
Delayed post intravenous contrast excretory phase CT scans may, on occasion, be
necessary to further delineate small ureteral stones and to differentiate them from
phleboliths in close proximity to the ureter or to assess unexpected renal parenchymal
Chapter 20 / Imaging of Urinary Stone Disease 389
abnormalities suspected on initial noncontrast scans. As with an IVU, a dense nephrogram
associated with delayed excretion of contrast and dilatation of the collecting system is
often associated with ureteral obstruction on post-contrast scans.
C
OMPUTED-TOMOGRAPHY SIGNS OF UROLITHIASIS AND OBSTRUCTION
Ureteral obstruction is associated with secondary signs on CT. These include unilat-
eral hydroureter and/or hydronephrosis. Subtle degrees of collecting system distention
or perinephric fat stranding are most easily recognized in or about the upper or lower
poles of the kidney. Perinephric or periureteral fat stranding may also be encountered
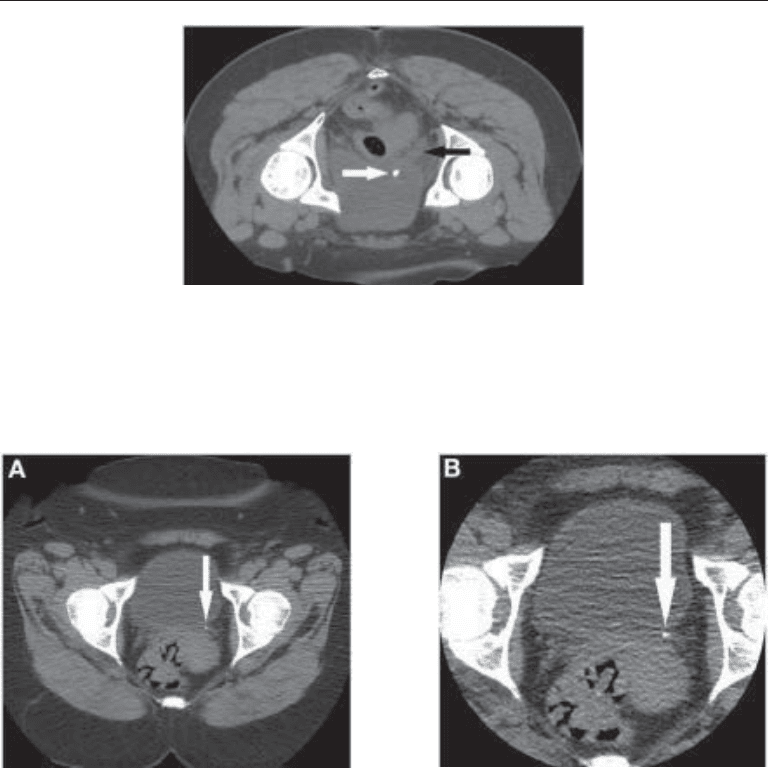
Fig. 18. (A) Nonenhanced 5–mm-thick CT section obtained on a multidetector CT scanner
showing a questionable calcific density (arrow) in the left ureterovesical junction. (B) Thin
section small field-of-view image reconstructed from the same dataset confirms a small stone
(arrow) in the left ureterovesical junction. The ability to retrospectively create such targeted high-
resolution reconstructions (while the raw data remains available) is one of the advantages of
multidetector CT scanners.
Fig. 17. Nonenhanced CT image demonstrating the advantage of prone positioning in the evalu-
ation of urinary stones. The distal right ureter (black arrow) is dilated to the level of a small stone
(white arrow) impacted in the ureterovesical junction. With a scan obtained in the supine position,
it could be difficult to distinguish a stone in the ureterovesical junction protruding into the bladder
from a stone that has passed from the ureter and was lying freely within the bladder.