Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

430 Section V • Gallbladder
OPEN CHOLECYSTECTOMY
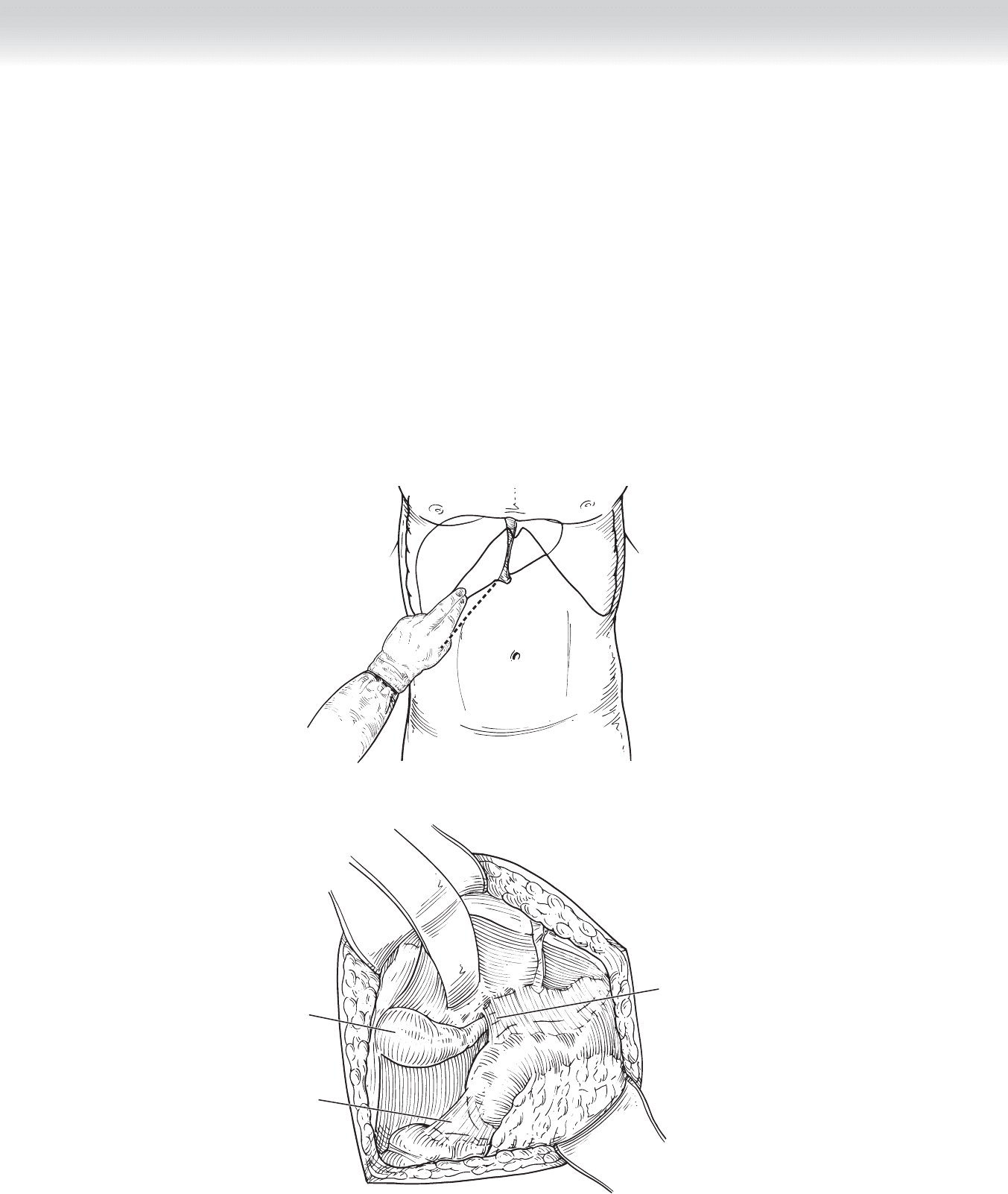
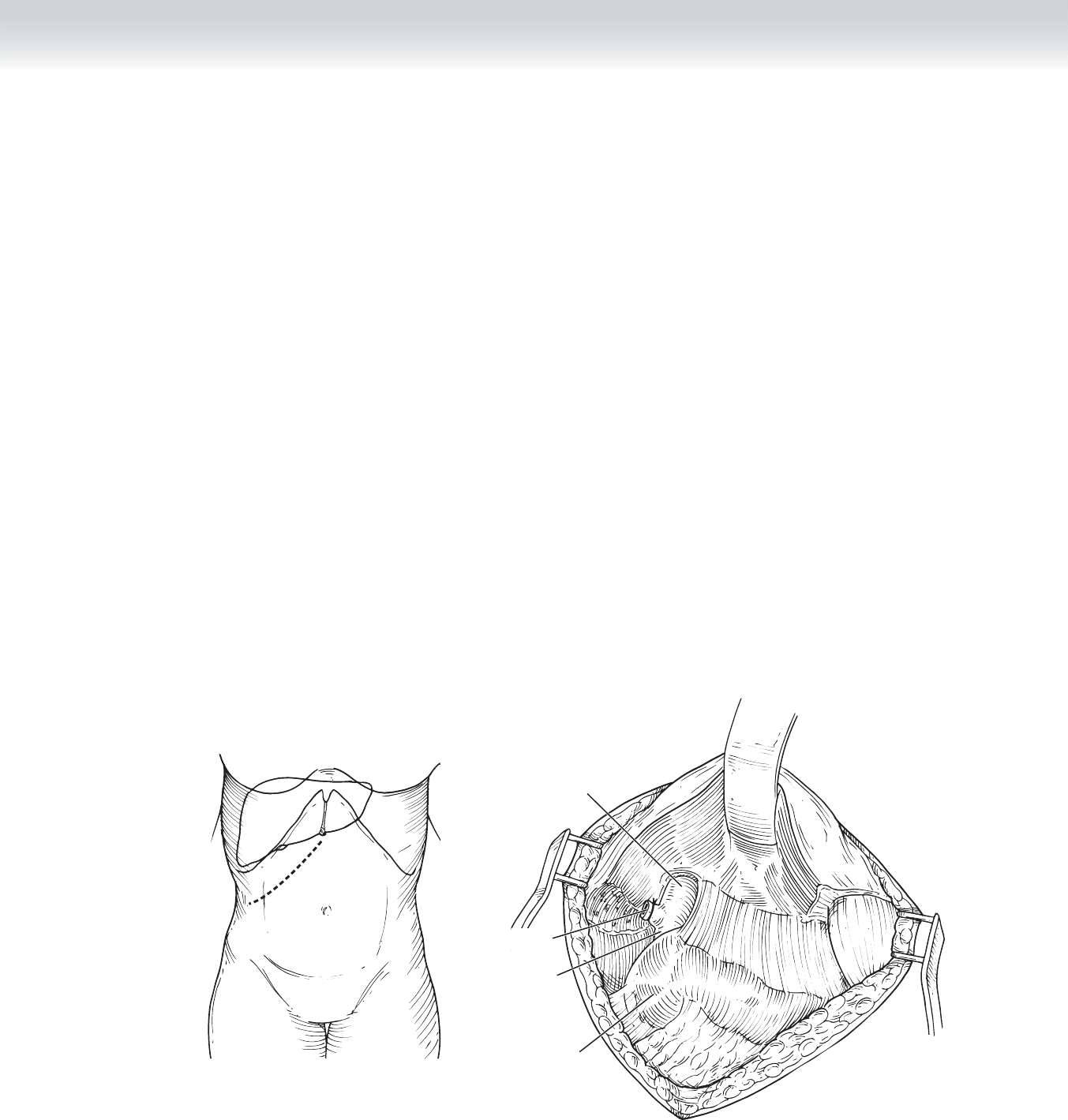
1. INCISION
◆ The incision for open cholecystectomy is typically made 2 fi ngerbreadths below the right
costal margin, although an upper midline incision can also be used (Figure 41-8, A).
◆ Retractors are placed to retract the skin, as well as to retract the liver superiorly
(Figure 41-8, B).
A
Gallbladder
Porta
hepatis
Hepatic
flexure
of colon
B
FIGURE 41 –8
CHAPTER 41 • Laparoscopic and Open Cholecystectomy 431
2. DISSECTION
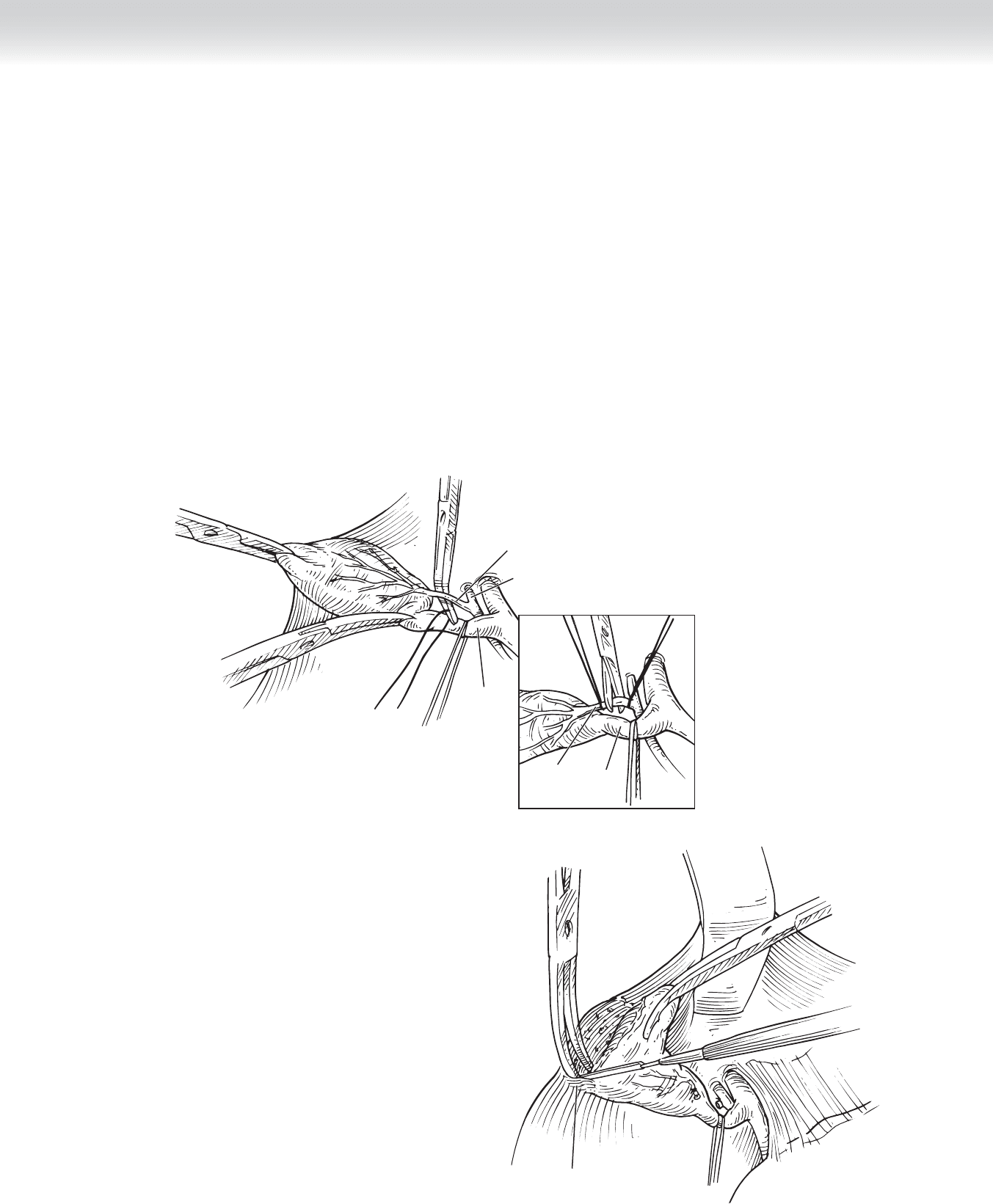
◆ A clamp is placed on the gallbladder fundus and used to retract the gallbladder superiorly
(Figure 41-9). A second clamp can be used to retract the infundibulum of the gallbladder
laterally (see Figure 41-9), exposing the triangle of Calot.
◆ Ideally, the cystic artery is identifi ed, circumferentially dissected, and ligated (see Figure 41-9)
before dissection of the gallbladder out of the gallbladder fossa. As in the laparoscopic case,
care should be taken not to injure the right hepatic artery.
◆ The gallbladder is then removed from the gallbladder fossa from the top down using
electrocautery (Figure 41-10).
Serosal
reflection
FIGURE 41 –10
Cystic
duct
Cystic artery
Right hepatic
artery
Cystic
duct
Cystic
artery
FIGURE 41 –9
432 Section V • Gallbladder
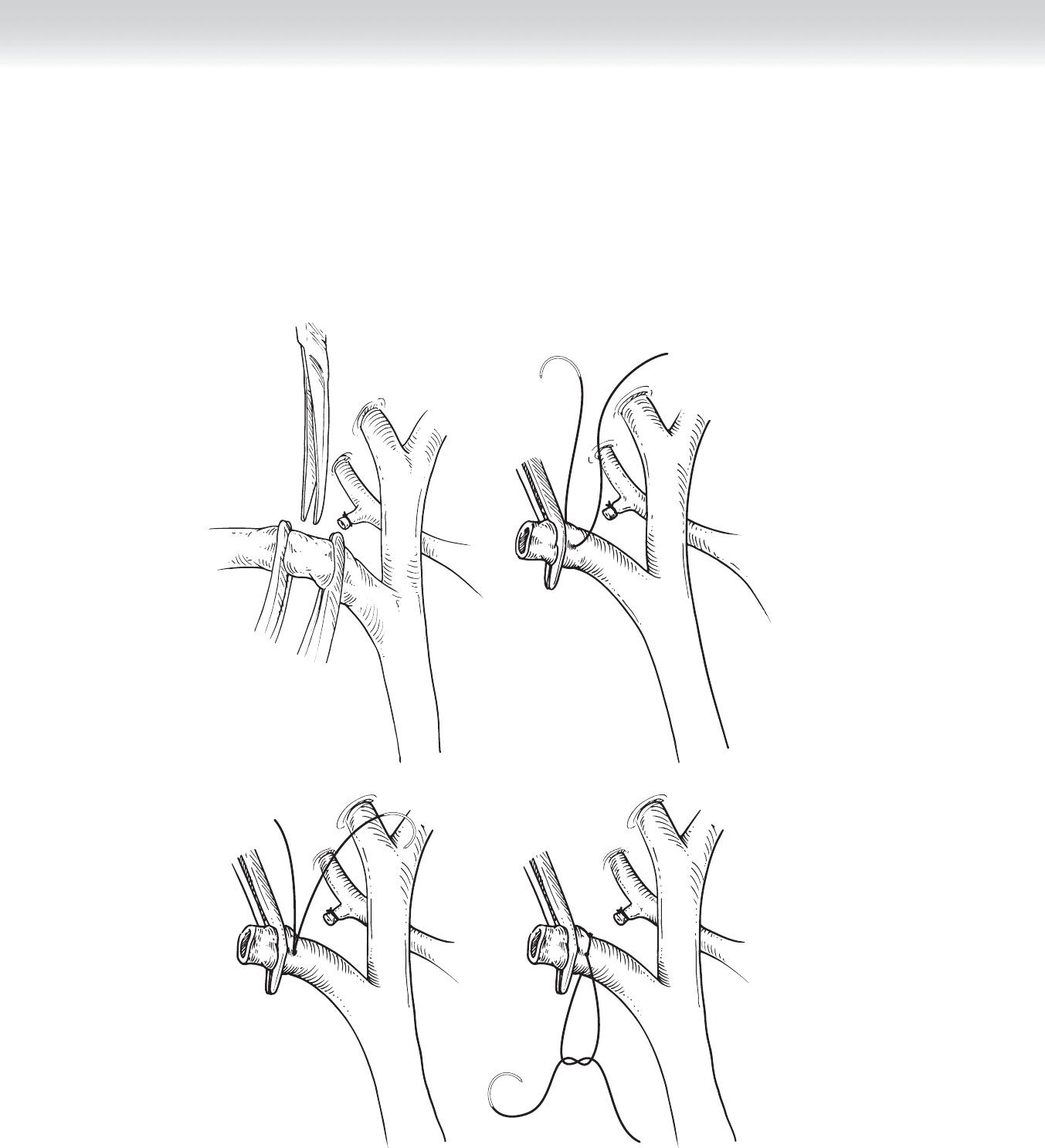
◆ Clamps are placed proximally and distally on the cystic duct. The cystic duct is divided
between the clamps (Figure 41-11, A), and the gallbladder is removed from the fi eld.
◆ The cystic duct stump is suture ligated using a 3-0 silk suture (Figures 41-11, B-D).
A B
C D
FIGURE 41 –11
CHAPTER 41 • Laparoscopic and Open Cholecystectomy 433
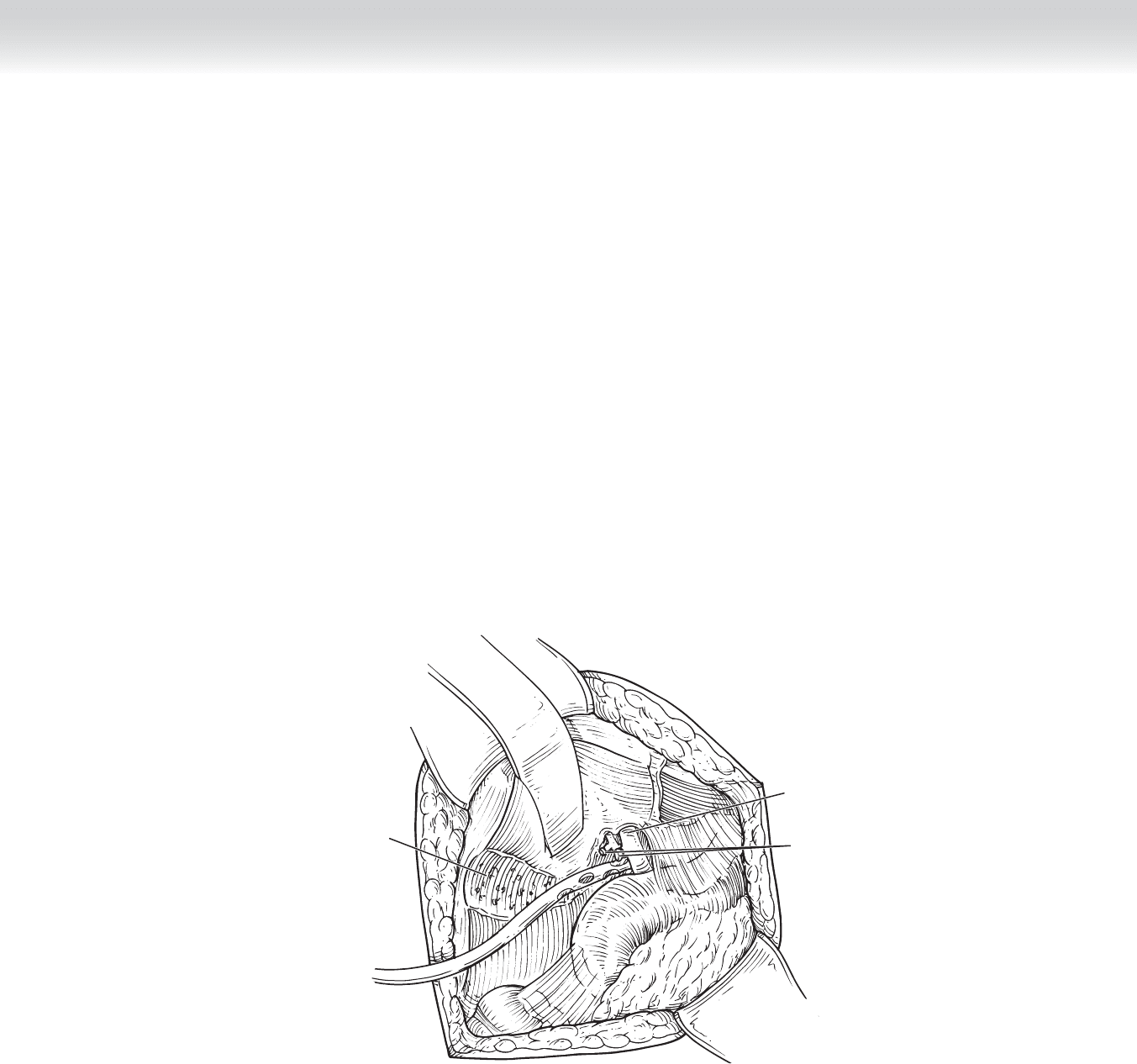
Common
hepatic duct
Cystic duct and
cystic artery
stumps
Gallbladder
fossa
FIGURE 41 –12
◆ The cystic duct and cystic artery stumps are examined for any signs of bile leakage or
bleeding (Figure 41-12). The abdomen is copiously irrigated with normal saline solution.
3. CLOSING
◆ The placement of closed suction drains is not always required. They are placed only if bile
leakage from the cystic duct stump is expected or observed. If bile leakage is observed, the
surgeon must rule out common bile duct injury.
◆ The fascia is closed in two layers using running or interrupted sutures.
◆ The skin is then closed with absorbable subcuticular sutures or skin staples.

434 Section V • Gallbladder
STEP 4: POSTOPERATIVE CARE (LAPAROSCOPIC AND OPEN CHOLECYSTECTOMY)
◆ Postoperative complications include hematoma, bleeding, or leakage from the cystic duct
stump.
◆ If a drain is placed operatively, the output should be monitored. If no bilious drainage is
observed at 24 to 48 hours, the drain can be removed.
◆ If bilious drainage is noted, this can initially be managed conservatively with continued
observation. Liver function tests should be performed to evaluate for bile duct injury. If
drainage persists, endoscopic retrograde cholangiopancreatography (ERCP) is indicated to
defi nitively rule out injury. In addition, a common bile duct stent placed via ERCP will also
treat persistent cystic duct leaks in the absence of common bile duct injury.
◆ Clear liquids can be started immediately postoperatively for both laparoscopic and open
cholecystectomy and generally advanced as tolerated. Patients undergoing open procedures
may have a longer time to return to regular diet.
◆ Patients are discharged home the same day after laparoscopic cholecystectomy and 2 to 3 days
after open cholecystectomy.
◆ Longer stay may be necessary in the setting of acute cholecystitis.
◆ For uncomplicated gallstone disease, antibiotics are not continued postoperatively.
STEP 5: PEARLS AND PITFALLS
◆ To avoid bile duct injury, it helps to retract the infundibulum of the gallbladder laterally to
open up the triangle of Calot and form a 90-degree angle of the cystic duct with the com-
mon hepatic duct. Pulling the infundibulum superiorly orients the cystic duct similar to the
common bile duct and can lead to injury.
◆ After dividing the cystic duct and cystic artery, it is useful to begin the dissection of the
gallbladder bluntly to make sure there are no ductal structures present.
◆ A 5-mm port and a 5-mm clip applier can be used at the epigastrium. If this is done, a 5-mm
camera will need to be present if a retrieval bag is going to be used to remove the gallbladder,
because this comes in only the larger size.
◆ Cholecystectomy can be performed from the top down in both the laparoscopic and the
open settings, although it is more diffi cult in the laparoscopic setting.

◆ The clips placed on the cystic duct and artery need to completely occlude the lumen. If this
is not possible on the cystic duct, an Endoloop can be placed. In this setting, the anatomy
should be reviewed to ensure that the cystic duct is ligated and the anatomy has not been
incorrectly identifi ed, because the clips are usually large enough to occlude the cystic duct.
◆ Cholangiogram can be performed routinely or selectively, based on the preference of the
operating surgeon.
◆ If common bile duct stones are identifi ed, a laparoscopic or open common bile duct
exploration can be performed. Alternatively, ERCP can be performed to clear the duct
postoperatively.
◆ Multiple previous abdominal surgeries, severe cardiac disease, and severe acute cholecystitis
are relative contraindications to laparoscopic cholecystectomy. When a patient has a history
of multiple previous abdominal surgeries, an open technique should be used to place the
initial umbilical port.
◆ When performing laparoscopic procedures, it is best to convert to an open procedure if
(1) there is uncontrolled bleeding; (2) safe laparoscopic access to the abdominal cavity can-
not be obtained; (3) the anatomy of the triangle of Calot cannot be clearly delineated; or
(4) injury to the common bile duct, small bowel, or any other structure is suspected. This
should not be considered a failure.
SELECTED REFERENCES
1. Jones DB, Maithel SK, Schneider BE (eds): Atlas of Minimally Invasive Surgery. Woodbury, Conn, Ciné-Med,
2006, pp 12-39.
2. Cameron JL: Atlas of Surgery, vol 1. Philadelphia, BC Decker, 1990, pp 2-9.
3. Posther KE, Pappas TN: Acute cholecystitis. In Cameron JL (ed): Current Surgical Therapy, 8th ed.
Philadelphia, Mosby, 2002, pp 385-391.
4. Hutter MM, Rattner DW: Open cholecystectomy: When is it indicated? In Cameron JL (ed): Current
Surgical Therapy, 8th ed. Philadelphia, Mosby, 2002, pp 400-401.
CHAPTER 41 • Laparoscopic and Open Cholecystectomy 435

436
STEP 1: SURGICAL ANATOMY
◆ A comprehensive understanding of the biliary, pancreatic, and foregut anatomy is critical
before performing any surgical procedure on the biliary tree, pancreatic duct and pancreas,
distal stomach, and duodenum.
◆ Figure 42-1, A demonstrates the location of the right subcostal incision 2 fi ngerbreadths
below the right costal margin.
◆ Figure 42-1, B shows the surgical anatomy after placement of retractors on the abdominal
wall and liver. In this case the patient had prior cholecystectomy. The common bile duct
travels posterior to the fi rst portion of the duodenum and through the head of the pancreas,
draining into the ampulla of Vater in the second portion of the duodenum. The hepatic ar-
tery lies medial to the common bile duct, and the portal vein is posterior to the common
bile duct.
◆ The diameter of the common bile duct needs to be at least 1.5 to 2.0 cm for a choledocho-
duodenostomy to be performed successfully. This is usually the case if the procedure is
being performed for retained common bile duct stones. Hepaticojejunostomy can be
performed in nondilated ductal systems, but it is more diffi cult.
STEP 2: PREOPERATIVE CONSIDERATIONS
1. PREPARATION
◆ The indications for side-to-side choledochoduodenostomy include retained common bile
duct stones after common bile duct exploration, primary common bile duct stones, and
recurrent common bile duct stones. The side-to-side choledochoduodenostomy enables
retained or new stones to pass spontaneously. It is especially useful in the setting of distal
common bile duct stricture.
CHAPTER
42
Choledochoduodenostomy and
Hepaticojejunostomy
Taylor S. Riall
CHAPTER 42 • Choledochoduodenostomy and Hepaticojejunostomy 437
A
Common
hepatic duct
Duodenum
Cystic duct
Common
bile duct
B
FIGURE 42 –1
◆ The indications for hepaticojejunostomy include benign distal biliary stricture, recurrent
cholangitis secondary to a stricture or stone disease, palliation of jaundice in patients with
unresectable periampullary cancer, and bile duct injury (usually iatrogenic). With bile duct
injuries, the duct is often normal caliber, making the operation more diffi cult.
◆ The patient is placed supine on the operating room table, with both arms extended.
◆ Subcutaneous heparin is given, and sequential compression devices are used to prevent
venous thromboembolism.
◆ A second-generation cephalosporin is used for antibiotic prophylaxis before skin incision
and redosed for the fi rst 24 hours.
◆ A Foley catheter is placed to monitor urine output.
◆ A nasogastric (NG) tube is placed to decompress the stomach. This is left in postoperatively.

438 Section V • Gallbladder
STEP 3: OPERATIVE STEPS
CHOLEDOCHODUODENOSTOMY
1. INCISION
◆ The operation is performed through a right subcostal incision (see Figure 42-1, A). It can
also be done using an upper midline incision.
2. DISSECTION
◆ Patients have often had previous cholecystectomy, and there may be adhesions between the
liver and the portal structures. The adhesions are dissected sharply using electrocautery or
scissors, or both.
◆ The duodenum and extrahepatic biliary tree are exposed (see Figure 42-1, B).
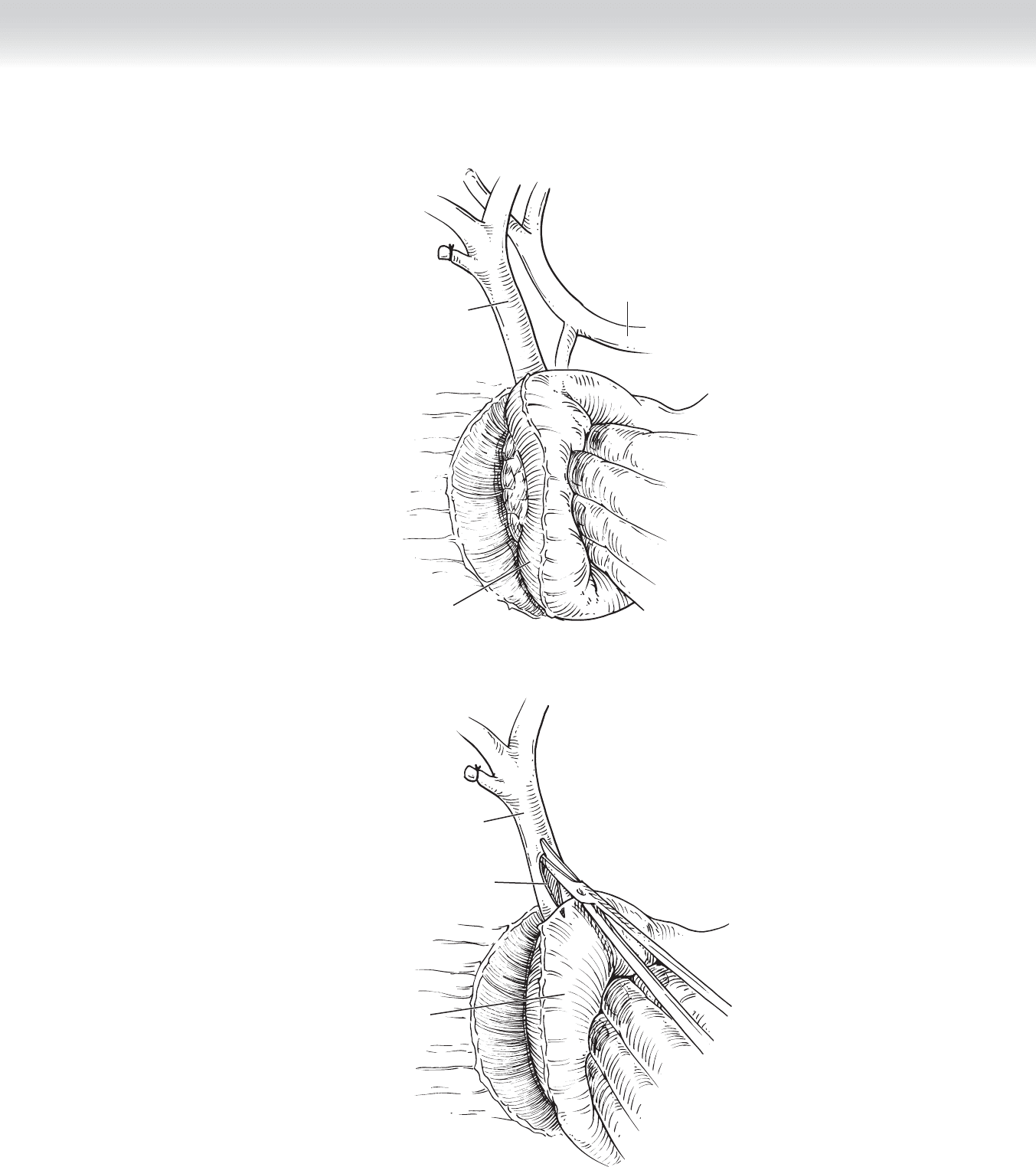
◆ The duodenum is kocherized out of the retroperitoneum (Figure 42-2). This may require
mobilization of the hepatic fl exure of the colon inferiorly. It is important to completely
mobilize the duodenum to perform the choledochoduodenostomy without tension.
◆ The duodenum is sharply dissected off the anterior surface of the distal common bile duct.
The common bile duct should be clearly exposed in the anterior and lateral surfaces.
◆ Using a no. 15 blade, an anterior choledochotomy is made in the common bile duct where
it courses posterior to the duodenum. The choledochotomy is extended to a length of
approximately 2 cm using Potts scissors (Figure 42-3). Stones are extracted if present.
CHAPTER 42 • Choledochoduodenostomy and Hepaticojejunostomy 439
Common
bile duct
Common
hepatic artery
Duodenum
FIGURE 42 –2
Common
bile duct
Choledochotomy
Kocherized
duodenum
FIGURE 42 –3