Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

440 Section V • Gallbladder
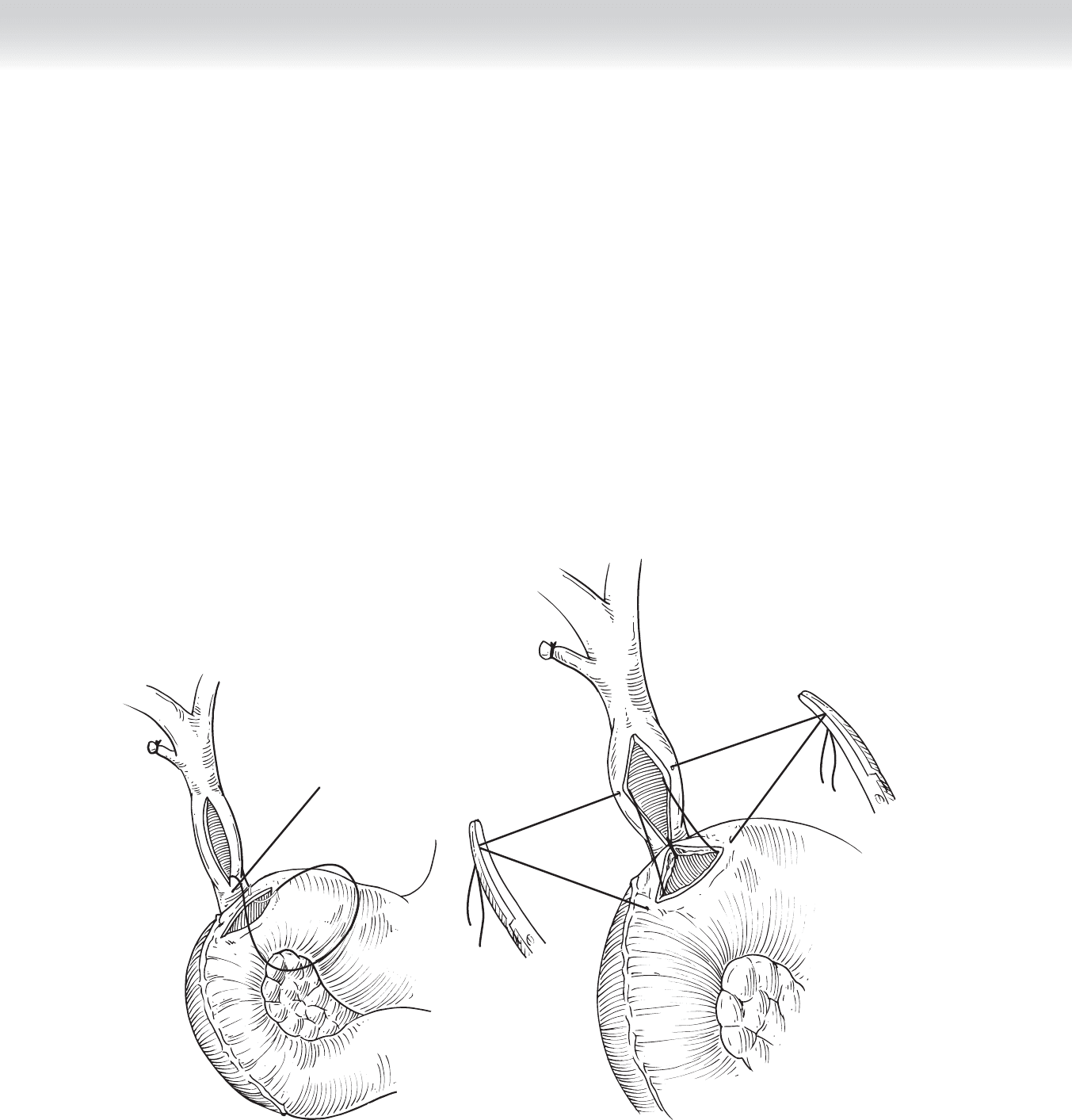
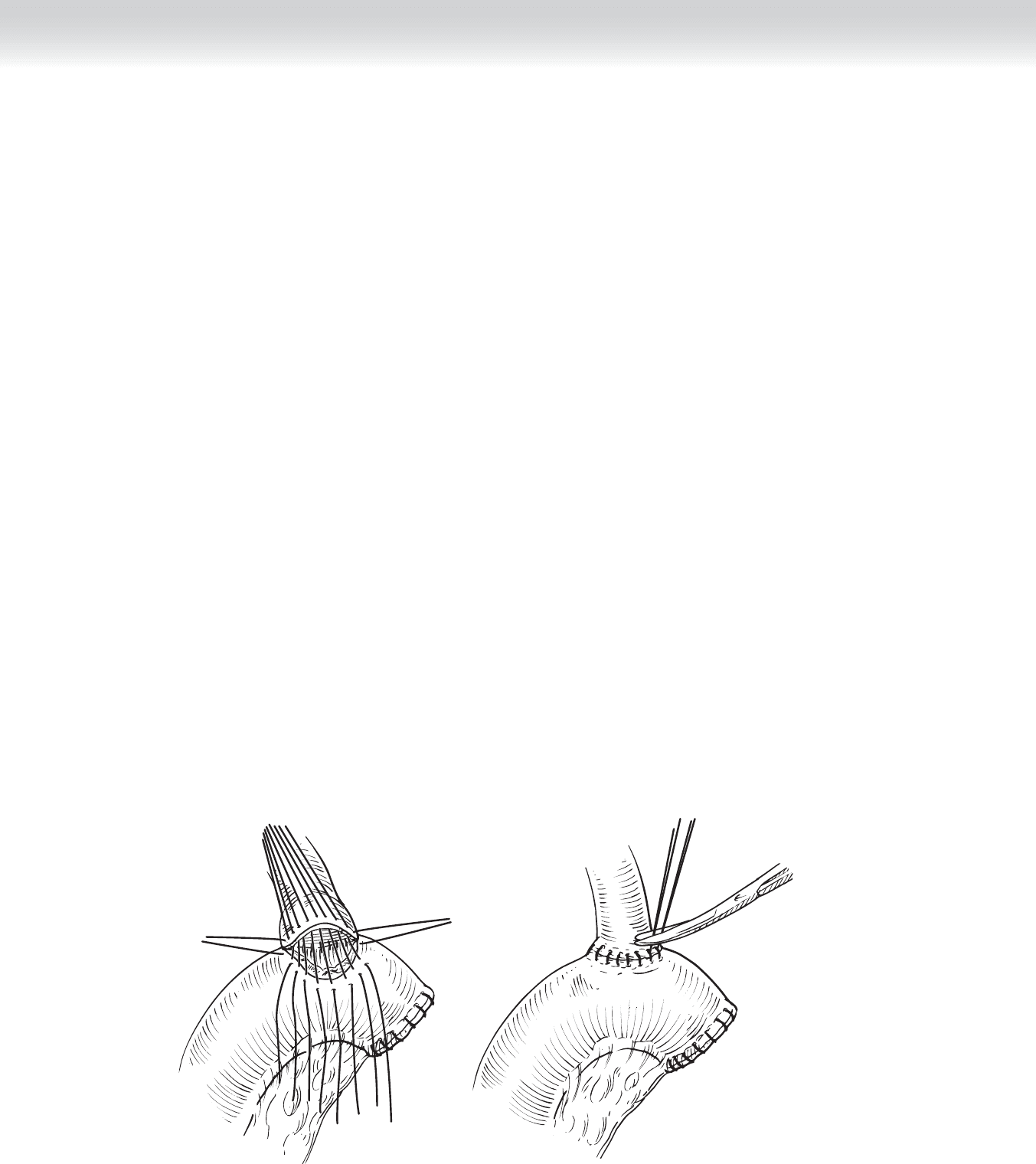
◆ A transverse duodenotomy is then performed adjacent to the choledochotomy using
electrocautery (Figure 42-4, A).
3. ANASTOMOSIS
◆ Absorbable 4-0 Vicryl sutures are used to perform a single-layer, side-to-side anastomosis. A
stitch is fi rst placed at the inferior apex of the choledochotomy, through the center of the
back wall of the duodenotomy with the knots placed on the outside. This apex suture is
tied (see Figure 42-4, A).
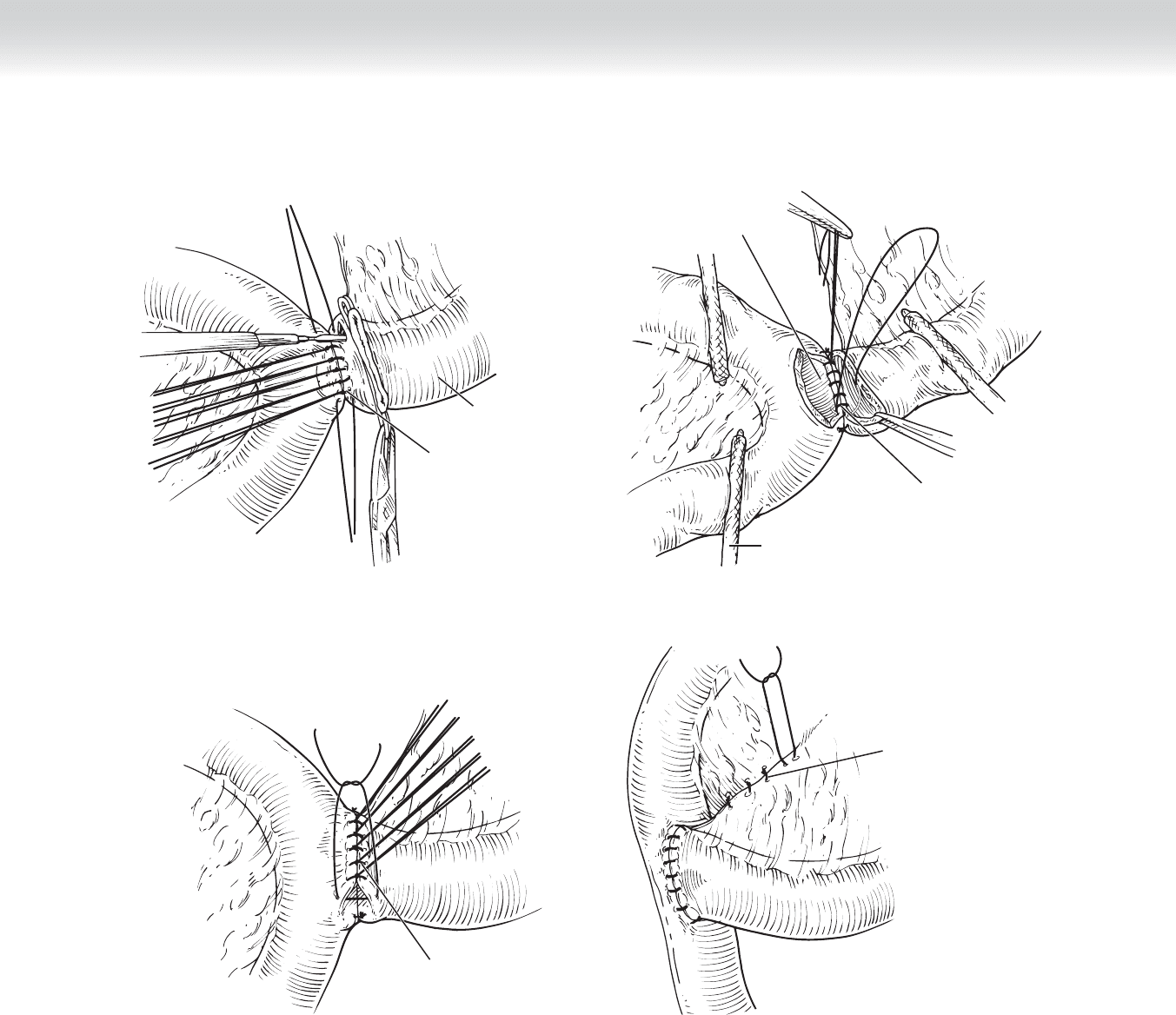
◆ Next, lateral stay sutures are placed. They pass from the midpoint of the choledochotomy
on each side to the respective end of the duodenotomy. These sutures are not tied and are
placed in hemostat clamps (Figure 42-4, B). Holding these stay sutures out laterally nicely
aligns the bile duct and duodenum for placement of the remaining sutures.
A B
FIGURE 42 –4
CHAPTER 42 • Choledochoduodenostomy and Hepaticojejunostomy 441
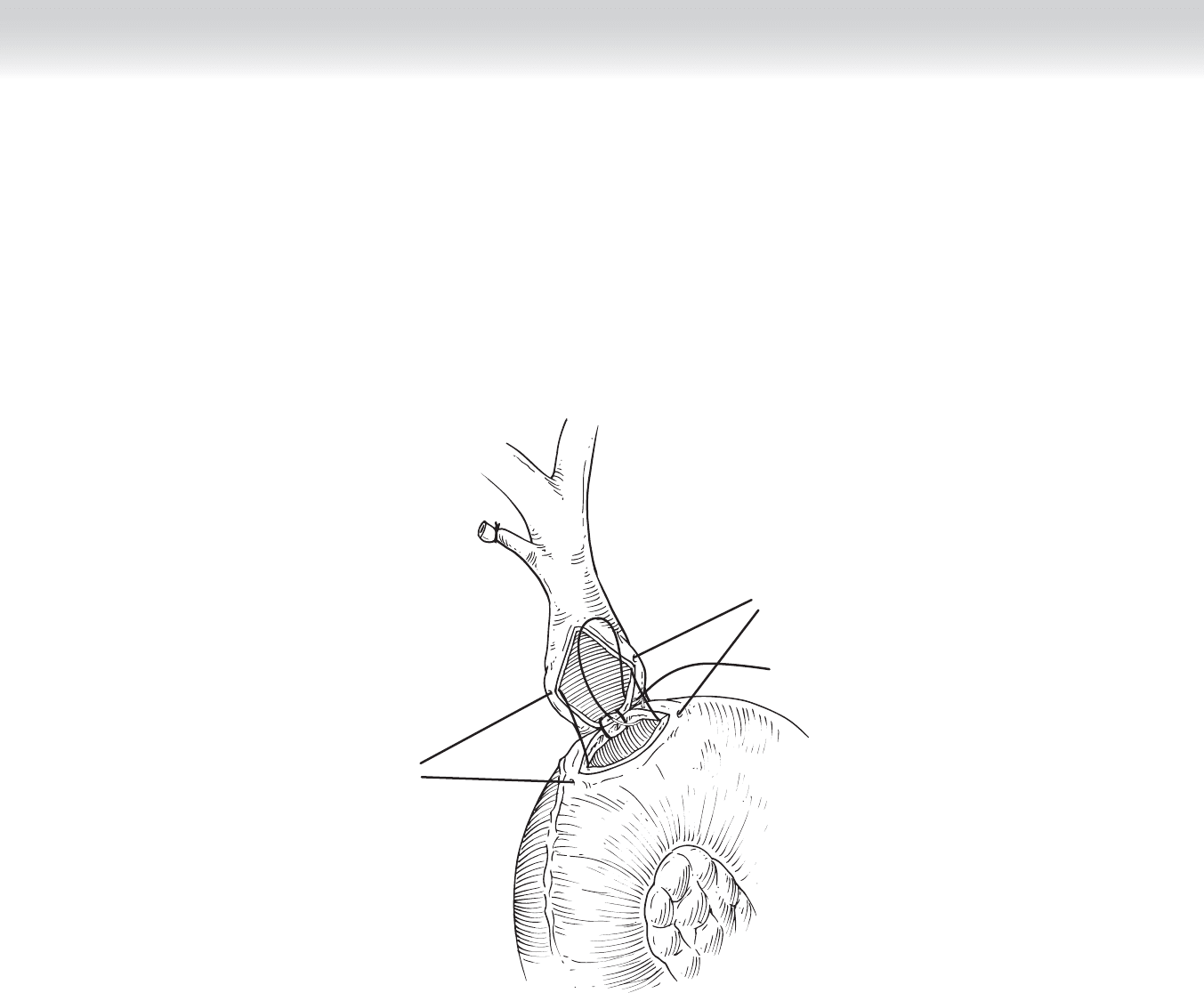
◆ The posterior row of sutures is then placed with the knots on the outside (Figure 42-5). These can
be tied and cut as the surgeon proceeds from the apex stitch to the lateral corner on each side.
FIGURE 42 –5
442 Section V • Gallbladder
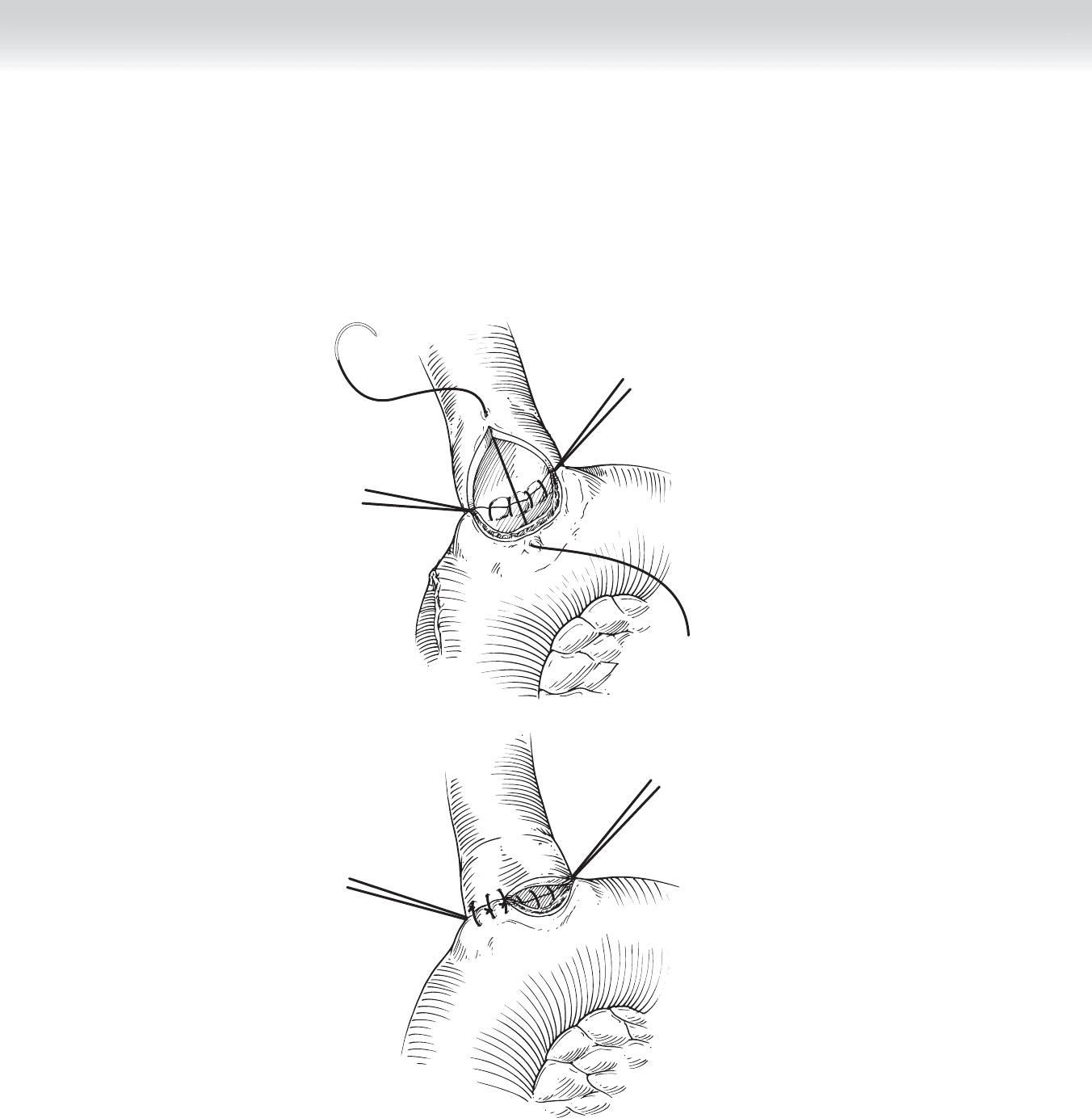
◆ The anterior row is then completed in similar fashion. An apex stitch is placed from the
midpoint of the duodenotomy to the superior apex of the choledochotomy (Figure 42-6, A).
The remaining stitches are placed in the anterior bile duct (Figure 42-6, B). To allow for
easier suture placement and careful approximation of the bile duct and duodenal mucosa, the
anterior sutures are all placed before they are tied down.
B
A
FIGURE 42 –6
CHAPTER 42 • Choledochoduodenostomy and Hepaticojejunostomy 443
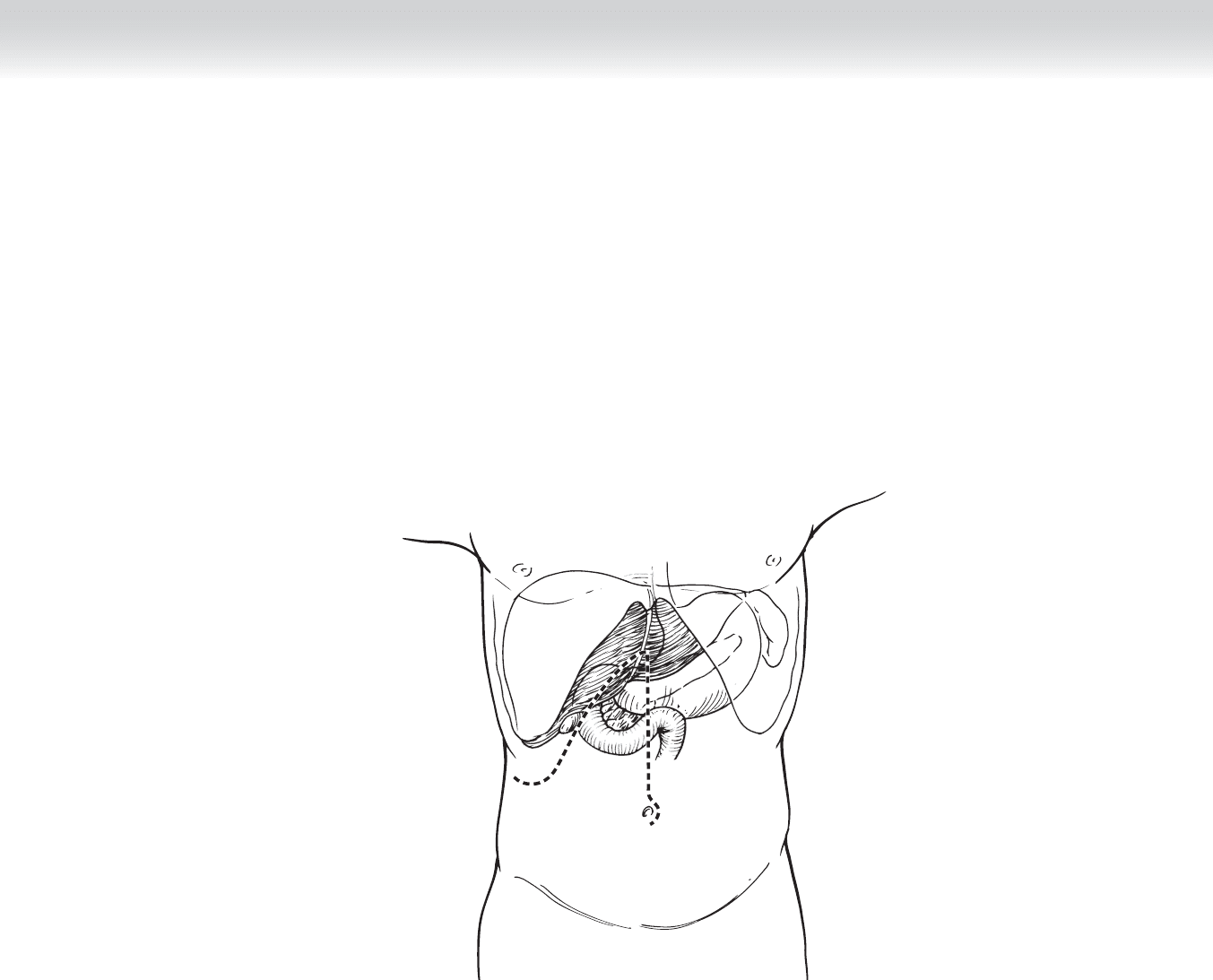
FIGURE 42 –7
HEPATICOJEJUNOSTOMY
1. INCISION
◆ The operation is performed through a right subcostal incision or an upper midline incision
(Figure 42-7).
444 Section V • Gallbladder
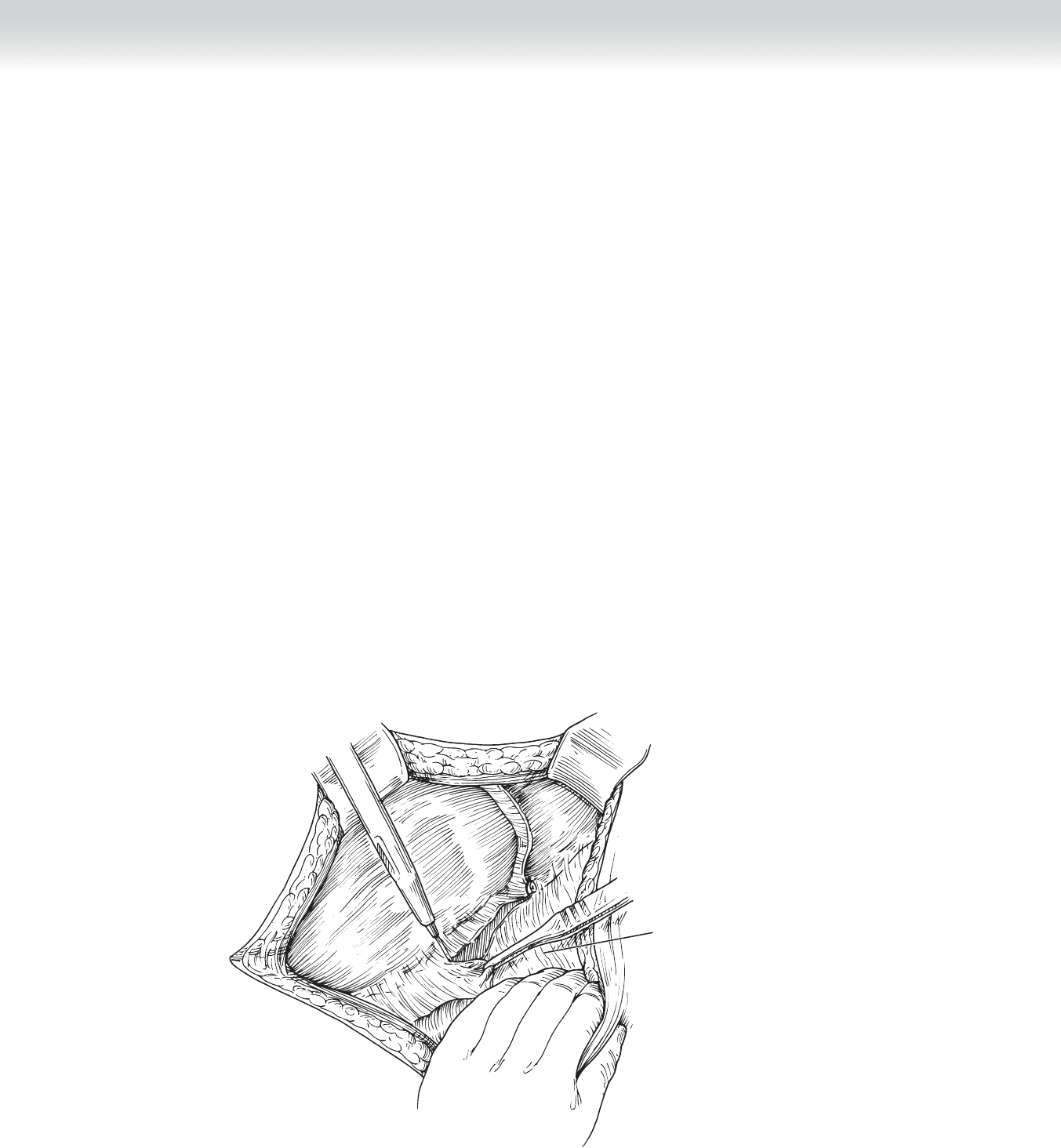
2. DISSECTION
◆ Patients have often had previous cholecystectomy and there may be adhesions between the
omentum and the liver and portal structures. These are dissected sharply using electrocau-
tery or scissors, or both (Figure 42-8).
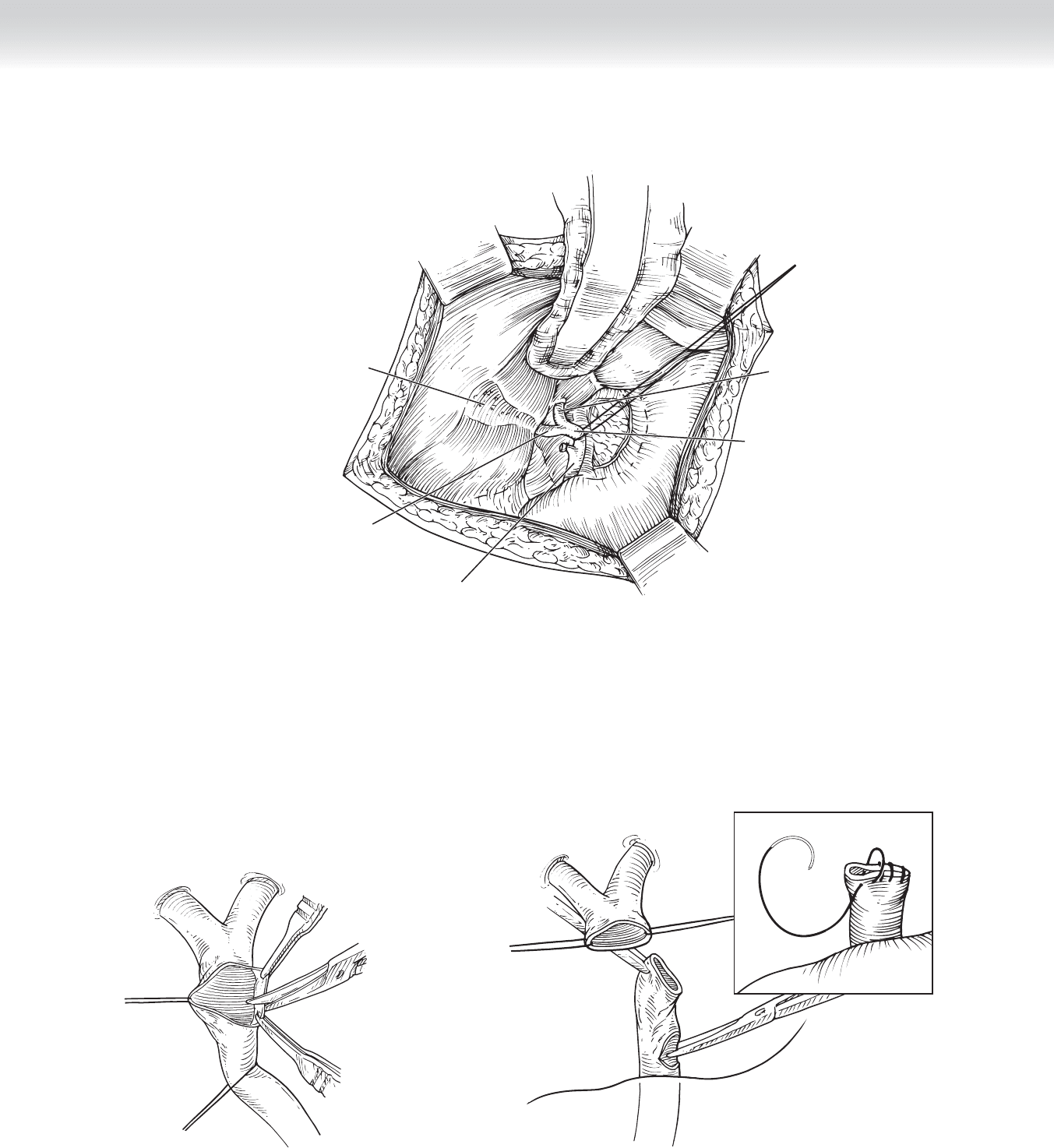
◆ The common bile duct/common hepatic duct are circumferentially dissected (Figure 42-9).
If a biliary stent has been previously placed, it can be palpated in the porta hepatis to help
identify the dissection plane. A vessel loop can be placed around the common bile duct,
which can facilitate dissection superiorly and inferiorly along the duct. The gallbladder has
often already been removed, but if it has not, cholecystectomy should be performed at the
same time.
◆ The common hepatic duct is then divided using electrocautery or scissors (Figure 42-10). If a
stricture is present, it is critical to divide the bile duct proximal to the stricture.
◆ Figure 42-11 shows excision of the strictured portion of the extrahepatic biliary tree if
present. The insert shows the ligation of the distal common bile duct with running absorb-
able suture.
Adhesions between
omentum and liver
FIGURE 42 –8
CHAPTER 42 • Choledochoduodenostomy and Hepaticojejunostomy 445
Gallbladder
fossa
Common
bile duct
Common
hepatic duct
Right
hepatic
duct
Left
hepatic
duct
FIGURE 42 –9
FIGURE 42 –10
FIGURE 42 –11
446 Section V • Gallbladder
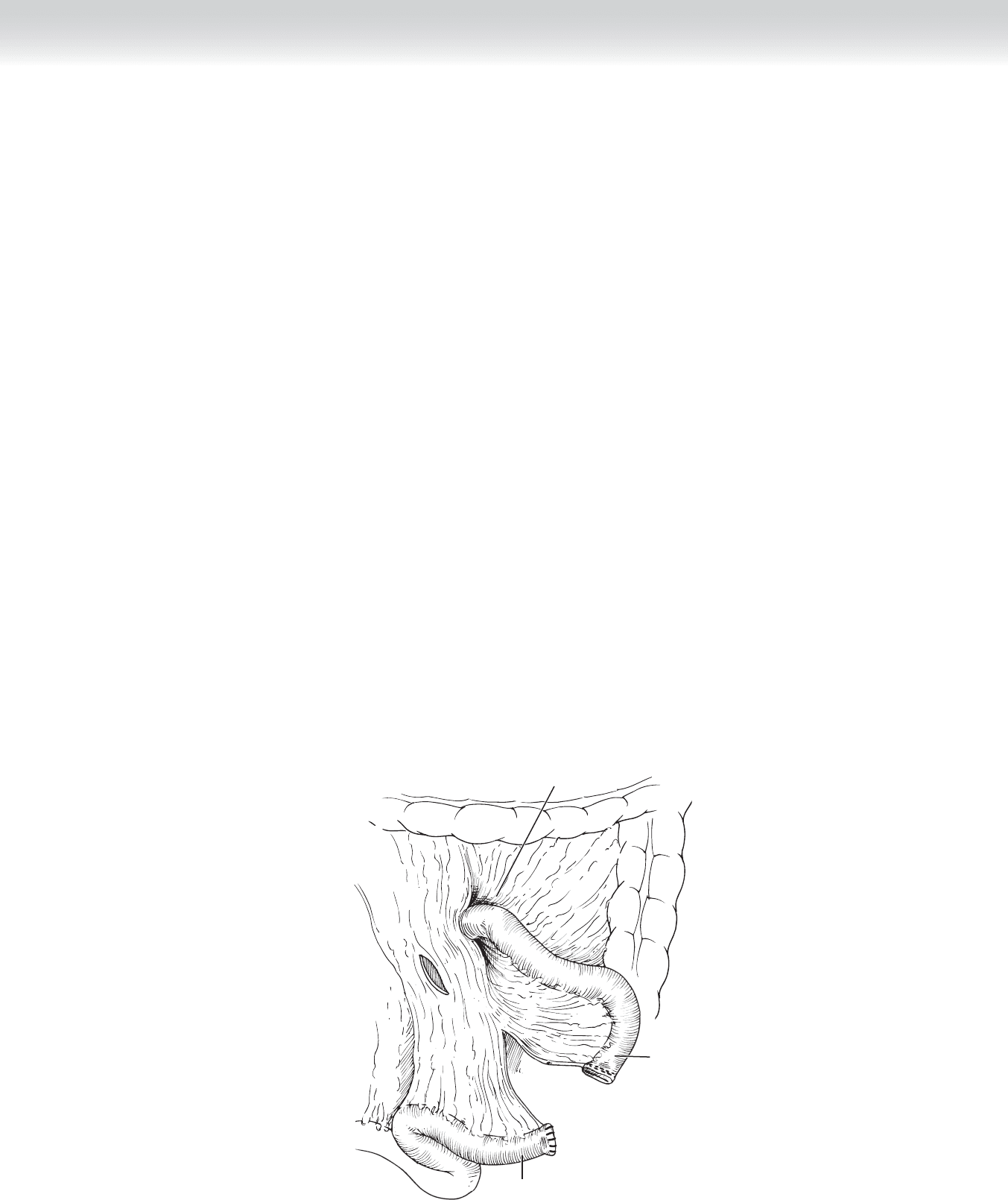
◆ After the bile duct has been divided and the distal end oversewn, a Roux-en-Y limb is created.
The transverse colon is lifted and the ligament of Treitz is identifi ed. The jejunum is divided
distal to the ligament of Treitz at a convenient arcade such that the Roux limb will easily reach
the bile duct. An incision is made in the transverse mesocolon above the duodenum and to
the right of the middle colic vessels (Figure 42-12).
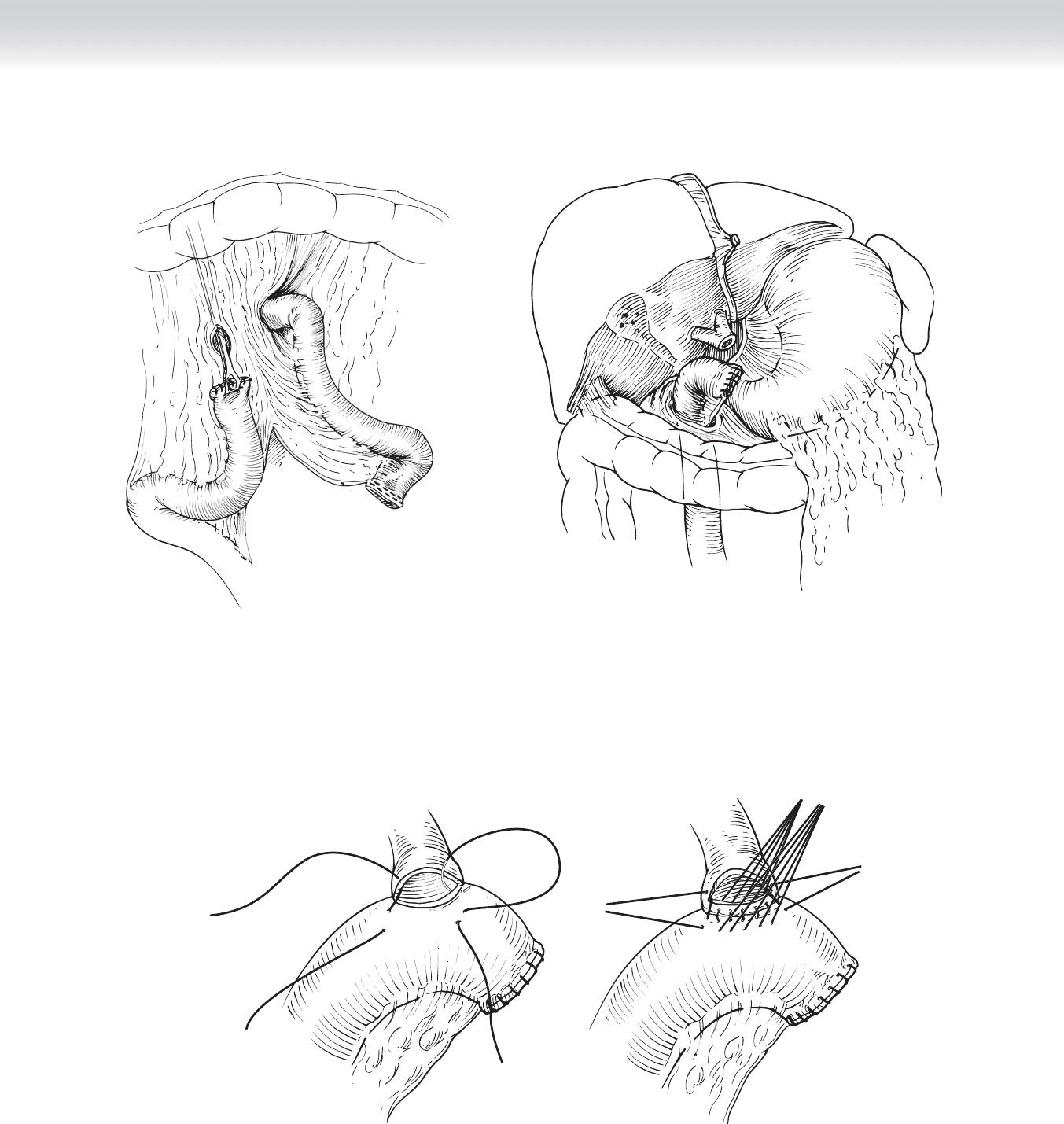
◆ The Roux limb is brought retrocolic through the transverse mesocolon on the right side for
the hepaticojejunostomy (Figures 42-13 and 42-14).
◆ The staple line of the jejunal limb is oversewn using interrupted 3-0 silk sutures.
3. ANASTOMOSIS
◆ Absorbable 4-0 Vicryl sutures are used to perform a single-layer, end-to-side hepaticojeju-
nostomy.
◆ Before making an enterotomy in the jejunum, the posterior layer of the anastomosis is per-
formed. Two corner sutures are placed fi rst. These sutures go through the jejunum, incor-
porating the submucosa. They are then placed inside out through the bile duct and secured
with hemostats (Figure 42-15, A).
◆ The back wall is then placed through the jejunum, incorporating the submucosa, and then
through the bile duct with the knots on the inside (Figure 42-15, B).
Ligament of Treitz
Proximal
jejunum
Distal
jejunum
FIGURE 42 –12
CHAPTER 42 • Choledochoduodenostomy and Hepaticojejunostomy 447
FIGURE 42 –13
FIGURE 42 –14
FIGURE 42 –15
A
B
448 Section V • Gallbladder
◆ After all the sutures in the posterior row have been placed, the jejunum is telescoped down
to the bile duct and all of the sutures are tied, including the corner sutures. The corner
sutures are placed back in hemostats and the other sutures are cut.
◆ After tying the posterior row of sutures, the surgeon makes a small enterotomy in the
jejunum (Figure 42-16, A). If a biliary stent is used, the surgeon places the distal end into
the jejunal limb at this point.
◆ The anterior layer of the anastomosis is completed using interrupted 4-0 Vicryl sutures
through both the jejunum and the bile duct (Figure 42-16, B).
◆ After construction of the hepaticojejunostomy, the surgeon perfoms a standard two-layer
end-to-side jejunojejunal anastomosis to restore bowel continuity. The posterior row of in-
terrupted 3-0 silk is shown in Figure 42-17, A. The running inner layer of 3-0 Vicryl is
shown in Figure 42-17, B. This is a running, locking suture in the posterior row and a
Connell stitch in the anterior row. Figure 42-17, C shows the interrupted layer of 3-0 silk
sutures used to complete the anterior row.
◆ Figure 42-17, D shows the completed anastomosis. Interrupted 3-0 silk sutures are used to
close the mesenteric defect at the jejunojejunal anastomosis (see Figure 42-17, D) and to
tack the Roux limb to the transverse mesocolon, where it passes retrocolic to prevent inter-
nal herniation.
A
B
FIGURE 42 –16
CHAPTER 42 • Choledochoduodenostomy and Hepaticojejunostomy 449
Proximal
Outer layer of
posterior row of
end-to-side
jejunojejunostomy
A
jejunum
Linen-shod
clamps
Inner layer of
posterior row
Enterotomy
B
Outer layer of
anterior row
C
Closure of
mesentery
D
FIGURE 42 –17