Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

450 Section V • Gallbladder
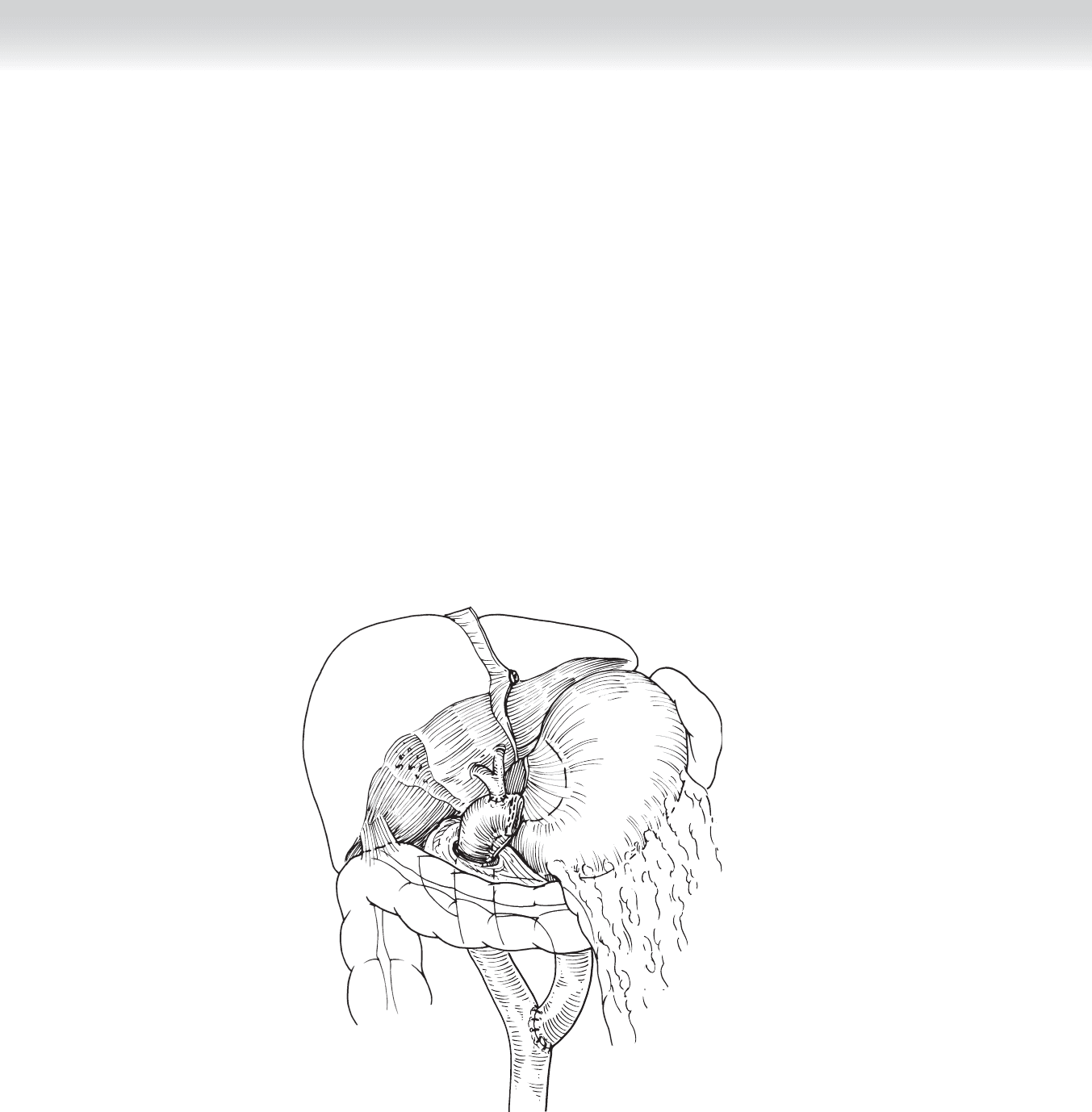
◆ The completed operation is shown in Figure 42-18.
4. CLOSING (CHOLEDOCHODUODENOSTOMY AND HEPATICOJEJUNOSTOMY)
◆ A closed suction drain is used to drain the choledochoduodenostomy or the hepaticojeju-
nostomy in the event of bile leakage.
◆ The fascia is closed in running or interrupted fashion per the preference of the surgeon.
Absorbable or permanent sutures can be used.
◆ The skin is closed with skin staples or absorbable subcuticular sutures.
FIGURE 42 –18

CHAPTER 42 • Choledochoduodenostomy and Hepaticojejunostomy 451
STEP 4: POSTOPERATIVE CARE (CHOLEDOCHODUODENOSTOMY
AND HEPATICOJEJUNOSTOMY)
◆ Postoperative complications include bile leak, stricture at the hepaticojejunostomy, cholan-
gitis, and hematoma/bleeding.
◆ If a percutaneous biliary stent was placed before surgery, it should initially be placed to
external drainage. Before removal of the drain, the biliary stent should be capped off, inter-
nalizing the drainage.
◆ The output from the operatively placed drain should be monitored. If no bilious drainage is
observed after 4 to 5 days (and after internalization of biliary drainage if stent is in place),
the drain can be removed.
◆ If bilious drainage is noted, it can initially be managed conservatively with continued obser-
vation. Large leaks may require the placement of a percutaneous biliary drain to divert the
bile fl ow externally while the anastomosis heals, if one was not present preoperatively.
◆ Biliary stents, if present before surgery or placed after, should be left in place at least
6 weeks before removal.
◆ An NG tube is kept in place the evening of surgery and removed on postoperative day 1.
◆ Clear liquids are started in 48 to 72 hours, and the diet is advanced as tolerated.
◆ The duration of stay is usually 5 to 8 days.
STEP 5: PEARLS AND PITFALLS
◆ In the past, percutaneous biliary stents were commonly placed before hepaticojejunostomy.
Many studies show that infectious complications are increased if a biliary stent is placed
preoperatively, presumably caused by bactobilia. However, if cholangitis is present preoper-
atively, a percutaneous or endoscopic stent is needed to relieve the obstruction and prevent
sepsis. Cholangitis is uncommon in malignant obstruction. The data were from patients
undergoing pancreaticoduodenectomy and have been extrapolated to hepaticojejunostomy
alone.
◆ Tumors arising at the confl uence of the right and left hepatic ducts require resection of the
extrahepatic biliary tree, including the confl uence, and require bilateral hepaticojejunosto-
mies for reconstruction. In this case, bilateral preoperative stents may make the small anas-
tomoses easier and prevent postoperative stricture formation.

452 Section V • Gallbladder
◆ Preoperative biliary stents may also be helpful in the event of common bile duct injury to
control leakage and make the anastomosis in a normal caliber bile duct easier.
◆ In the nondilated bile duct, it is best to perform the enterotomy in the jejunal limb before
performing the posterior row of the hepaticojejunostomy to prevent occlusion of the lumen
by excess tissue. This is not a problem in dilated bile ducts.
◆ With distal common bile duct stricture, malignancy should be considered and ruled out
before biliary bypass.
SELECTED REFERENCES
1. Cameron JL: Atlas of Surgery, vol 1. Philadelphia, BC Decker, 1990, pp 28-57.
2. Sohn TA, Yeo CJ, Cameron JL, et al: Do preoperative biliary stents increase postoperative complications?
J Gastrointest Surg 2000;4:258-267.
3. Jagannath P, Dhir V, Shrikhande S, et al: Effect of preoperative biliary stenting on immediate outcome after
pancreaticoduodenectomy. Br J Surg 2005;92:256-361.
4. Povoski SP, Karpeh MS, Conlon KC, et al: Association of preoperative biliary drainage with postoperative
outcome following pancreaticoduodenectomy. Ann Surg 1999;230:131-142.
453
STEP 1: SURGICAL ANATOMY
◆ A comprehensive understanding of the biliary, pancreatic, and foregut anatomy is critical
before performing any surgical procedure on the biliary tree, pancreatic duct, pancreas,
distal stomach, or duodenum.
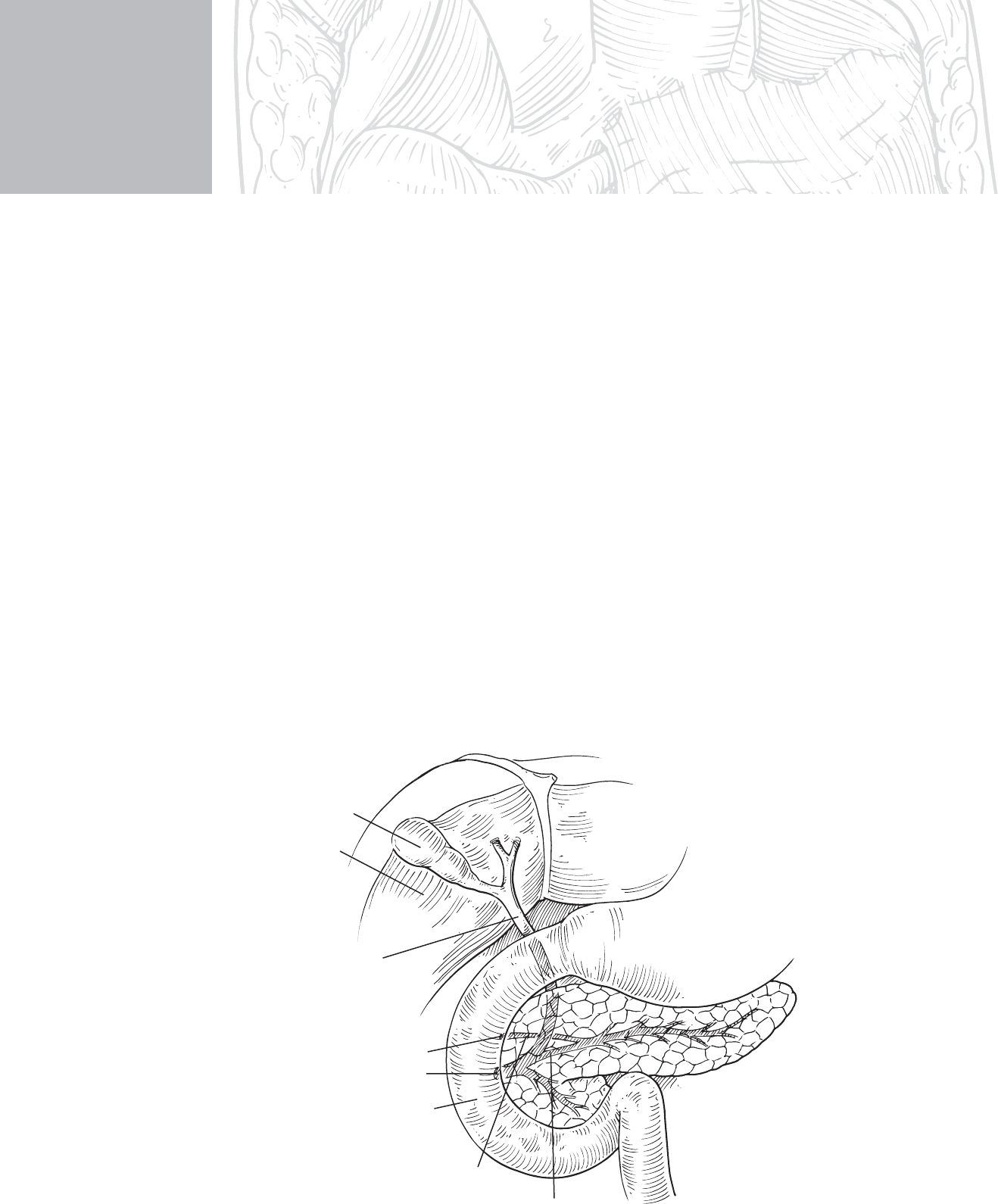
◆ Figure 43-1 illustrates the normal pancreaticobiliary anatomy. Structures that must be
considered during sphincteroplasty include the gallbladder, the common bile duct (CBD),
the head of the pancreas, the main and minor pancreatic ducts, the ampulla of Vater (major
papilla), the minor papilla, and the duodenum. It is critical to understand the complex
relationship of these structures to one another, with the CBD beginning at the confl uence of
the cystic duct and common hepatic duct. The CBD runs through the head of the pancreas
and drains into the duodenum at the ampulla of Vater. In most patients the main pancreatic
duct joins the distal CBD before draining into the ampulla of Vater, forming a common
channel.
CHAPTER
43
Sphincteroplasty
Taylor S. Riall
Liver
Gallbladder
Common
bile duct
Main
pancreatic duct
Minor
pancreatic
duct
Ampulla of Vater
Minor papilla
Duodenum
FIGURE 43–1

454 Section V • Gallbladder
◆ Figure 43-2 represents pancreas divisum, the most common congenital anomaly of the
pancreatic ductal system. Pancreas divisum occurs in approximately 6% to 7% of healthy
patients at autopsy. It occurs in up to 10% to 20% of patients with recurrent acute pancre-
atitis. Pancreas divisum results from a failure of fusion of the dorsal pancreatic duct and the
duct draining the uncinate process and head of pancreas. The result is that the major por-
tion of the drainage of the exocrine pancreas is through the minor papilla, with only the
duct to the uncinate process draining to the ampulla of Vater. The role of this anomaly in
causing pancreatitis is unclear, but it is thought to be the cause in a small number of
patients with recurrent acute pancreatitis, pancreas divisum, and a stenotic minor papilla.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ The use of transduodenal sphincteroplasty is controversial in many settings. For many
indications it has been replaced by endoscopic sphincterotomy via endoscopic retrograde
cholangiopancreatography (ERCP). The decision to perform this operation depends on the
surgeon’s expertise, the clinical situation, and the expertise of local gastroenterologists.
◆ Transduodenal sphincteroplasty has been used in a variety of settings. The indications for
transduodenal CBD sphincteroplasty include:
◆ Calculous disease of the biliary tract not amenable to stone removal via ERCP.
◆ Sphincteroplasty should be performed if the surgeon believes there are retained stones
after CBD exploration.
◆ Sphincterotomy and sphincteroplasty can be used to retrieve stones impacted in the distal
CBD that cannot be removed with choledochotomy and CBD exploration.
◆ Sphincteroplasty can be used to explore the CBD with a small-caliber duct in which
choledochotomy and T-tube placement may be diffi cult.
◆ Treatment of recurrent and acute pancreatitis with ampullary stenosis identifi ed and no
other cause of pancreatitis identifi ed; considered a rare indication.
◆ The use of sphincteroplasty and pancreatic duct septotomy for postcholecystectomy
syndrome remains controversial.
◆ CBD sphincteroplasty and pancreatic duct septotomy are often performed with minor
papilla sphincteroplasty (see later) to ensure adequate drainage in patients with symp-
tomatic pancreas divisum.
◆ The indications for minor papilla sphincteroplasty include:
◆ Recurrent acute pancreatitis (abdominal pain and hyperamylasemia)
◆ Pancreas divisum with no other obvious cause of acute pancreatitis identifi ed
STEP 3: OPERATIVE STEPS
1. INCISION
◆ The patient is placed supine on the operating table, with both arms extended out to the side.
◆ A fl uoroscopy table or table with radiographic capability is needed for possible intraopera-
tive cholangiography.
CHAPTER 43 • Sphincteroplasty 455
◆ The operation can be performed through a right subcostal or upper midline incision.
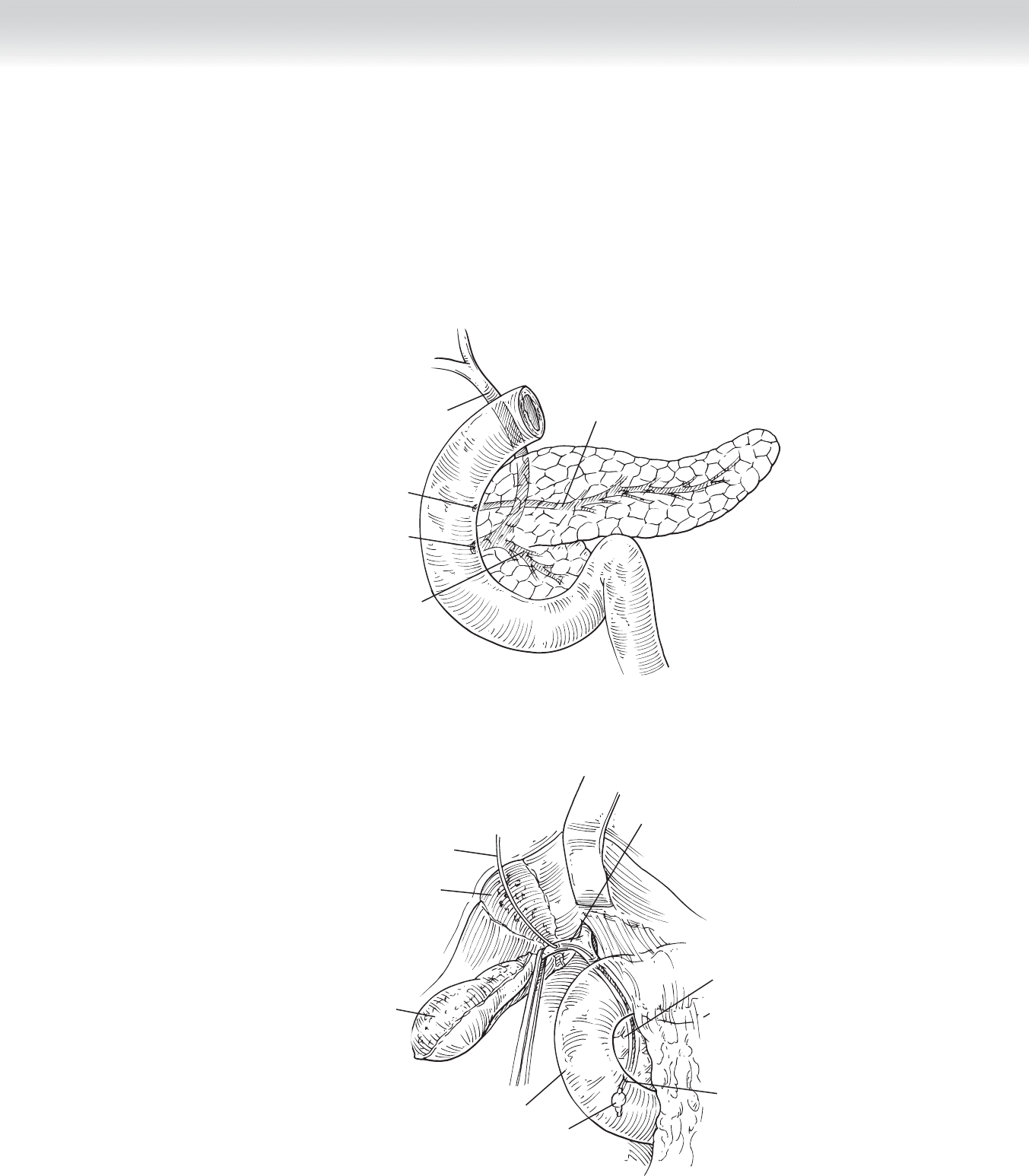
◆ In addition to the abdominal wall being retracted, the liver should be retracted superiorly,
exposing the gallbladder, portal structures, and duodenum (Figure 43-3).
Common
bile duct
Main
pancreatic duct
Pancreatic duct to
uncinate process
Ampulla of Vater
Minor papilla
FIGURE 43 –2
Biliary balloon
catheter
Cystic duct
Head of
pancreas
Ampulla
of Vater
Balloon inflated in duodenum
Duodenum
Mobilized
gallbladder
Gallbladder
fossa
FIGURE 43 –3

456 Section V • Gallbladder
2. DISSECTION
◆ If the gallbladder is in place, a cholecystectomy is performed by dissecting the gallbladder
out of the gallbladder fossa, from the fundus down to the cystic structures (see Figure 43-3).
The cystic artery is identifi ed and ligated.
◆ The cystic duct is then opened and a biliary balloon catheter is placed into the CBD from
the cystic duct. Cholangiography, if indicated, is easily performed at this point. The catheter
should exit into the duodenum at the ampulla of Vater.
◆ At this point the duodenum should be mobilized out of the retroperitoneum using the
Kocher maneuver. Then the balloon should be infl ated and pulled back fl ush to the
ampulla of Vater and easily palpated (see Figure 43-3).
◆ After palpating the balloon on the biliary catheter, the balloon is advanced into the duode-
num. Two 3-0 silk stay sutures are placed to the right and left of where the duodenotomy
will be performed. A longitudinal duodenotomy is made at the site of initial palpation right
over the ampulla of Vater (Figure 43-4). This can be done with electrocautery.
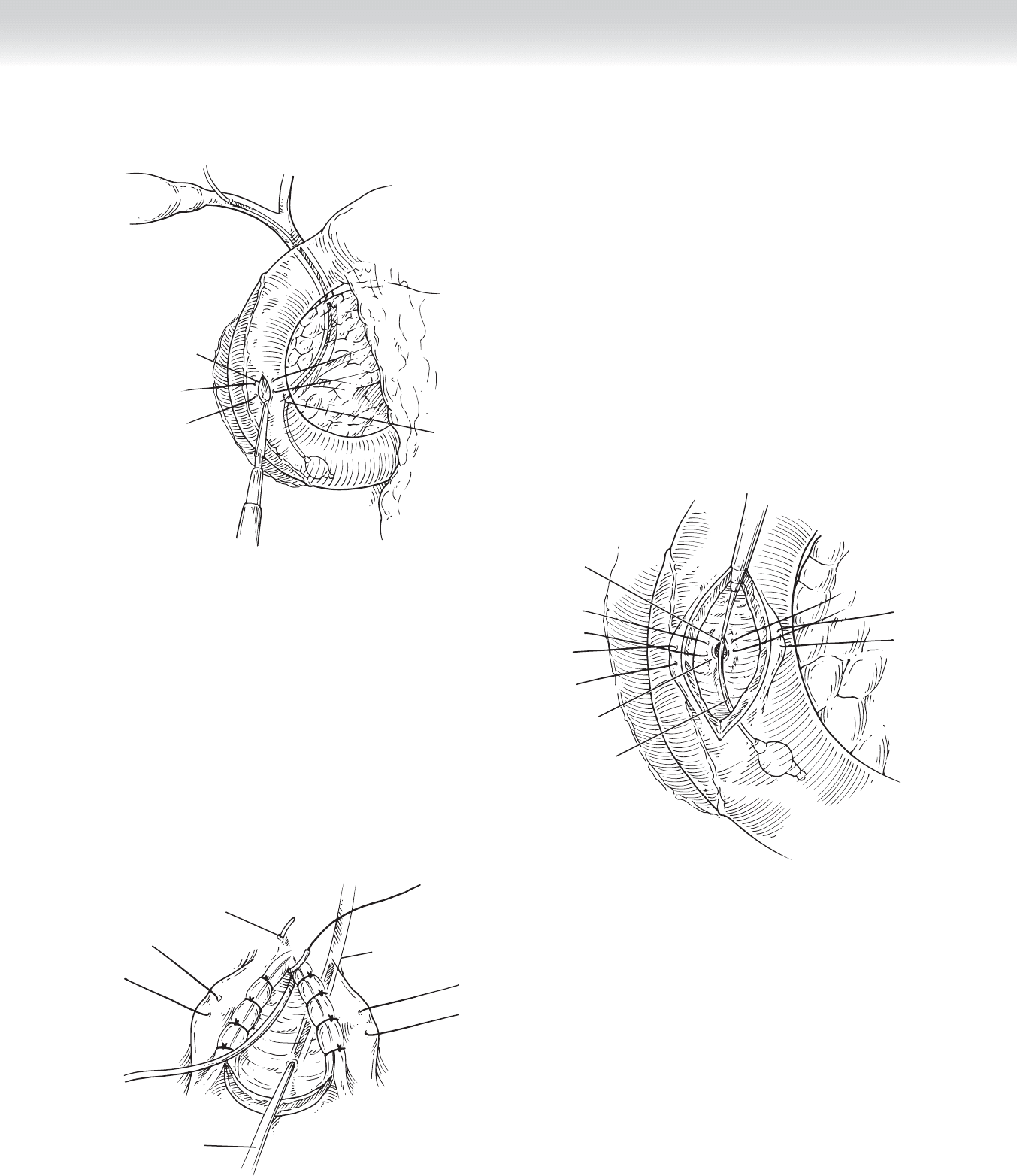
◆ The surgeon can then place his or her fi nger in the duodenotomy and palpate the balloon
and ampulla of Vater. The duodenotomy is then extended distally for adequate exposure of
the ampulla (Figure 43-5).
◆ Absorbable 5-0 sutures are then placed medial and lateral to the exiting biliary catheter at
the ampulla of Vater (see Figure 43-5).
◆ Using the biliary catheter for guidance, the surgeon performs a sphincterotomy of the ampulla
of Vater using electrocautery (see Figure 43-5). This should be performed slowly, 3 to 4 mm
at a time for a total length of 1 to 2 cm. The length of the sphincterotomy will vary depending
on the indication.
◆ After the sphincterotomy is performed, the CBD mucosa is approximated to the duodenal
mucosa using interrupted 5-0 absorbable sutures. The apex suture is shown in Figure 43-6,
with several other sutures already in place.
◆ Once the CBD is opened, the pancreatic duct orifi ce can be identifi ed, and a lacrimal duct
probe can be placed into the duct (see Figure 43-6).
CHAPTER 43 • Sphincteroplasty 457
Balloon
advanced
Duodenotomy
Ampulla
of Vater
FIGURE 43 –4
Biliary balloon
catheter
Papillotomy of
ampulla of Vater
Ampulla
of Vater
FIGURE 43 –5
Main pancreatic
duct
Apex suture
Probe in
pancreatic duct
FIGURE 43 –6

458 Section V • Gallbladder
◆ To ensure adequate drainage of the pancreatic duct, a pancreatic duct septotomy can be
performed over the probe (Figure 43-7).
◆ In the case of pancreas divisum, the duodenotomy may need to be extended proximally on
the duodenum to identify the minor papilla. In cases where this is diffi cult to identify, secre-
tin can be given to stimulate pancreatic secretion and aid in identifi cation.
◆ The minor papilla is small and can be diffi cult to cannulate. A small lacrimal duct probe
should be used and inserted atraumatically to prevent hematoma at the minor papilla
(Figure 43-8).
◆ After cannulation, a papillotomy can be performed over the probe using electrocautery
similar to performing the sphincterotomy at the major papilla.
◆ The pancreatic ductal mucosa is approximated to the duodenal mucosa using 5-0 absorbable
suture, similar to the approximation of the CBD to the mucosa after ampulla of Vater
sphincteroplasty.
◆ After the sphincteroplasty is completed, the biliary catheter can be retracted and a cholan-
giogram performed if necessary.
◆ The biliary catheter is then removed and the cholecystectomy is completed by ligating the
cystic duct distal to the ductotomy made for the biliary balloon catheter, dividing the cystic
duct, and removing the gallbladder from the fi eld.
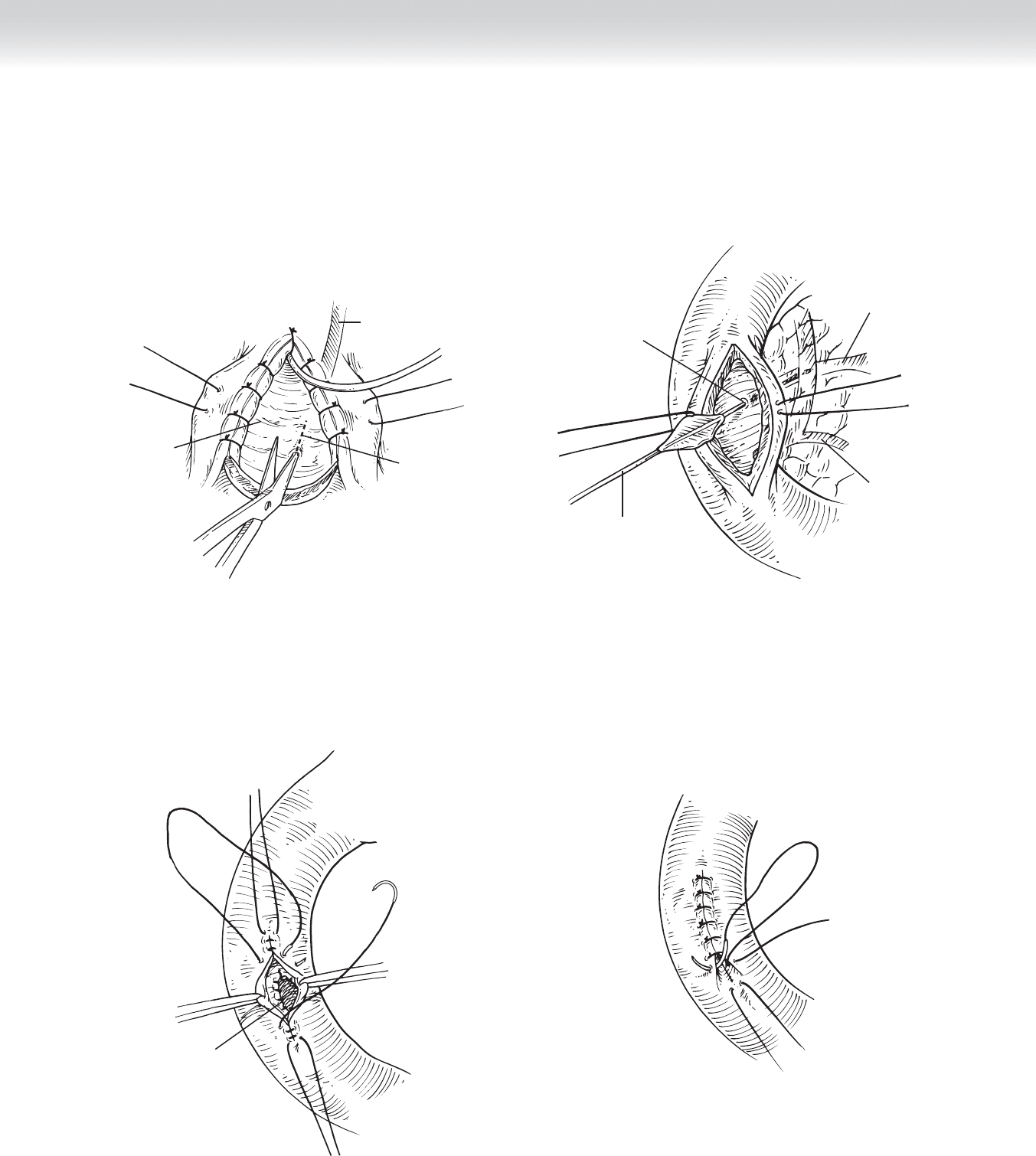
◆ The duodenotomy is then closed longitudinally in two layers. Care must be taken not to
narrow the duodenal lumen. Stay sutures of 3-0 silk are placed at the most proximal and
distal points of the duodenotomy. The fi rst layer is performed with absorbable 3-0 suture
in Connell fashion (Figure 43-9).
◆ The outer layer is closed in interrupted fashion using 3-0 silk suture (Figure 43-10).
◆ A closed-suction drain is placed to drain the duodenotomy.
CHAPTER 43 • Sphincteroplasty 459
Pancreatic duct
septotomy
Common
bile duct
Pancreatic duct
FIGURE 43 –7
Main
pancreatic duct
Duct to
uncinate
process
Minor papilla
Lacrimal
duct probe
FIGURE 43 –8
Sphincteroplasty
FIGURE 43 –9
FIGURE 43 –10