Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.


3. CLOSING
◆ The closed-suction drain is brought out through the anterior abdominal wall on the right
side, with care taken to avoid injury to the epigastric vessels.
◆ After irrigation is completed and hemostasis is ensured, fascial closure is performed per sur-
geon preference. Running or interrupted and permanent or absorbable sutures may be used
per surgeon preference.
◆ The skin is closed with a 4-0 Monocryl subcuticular suture or skin staples.
STEP 4: POSTOPERATIVE CARE
◆ Postoperative complications included hematoma, bleeding, or leakage from the duodenotomy.
◆ The output from the operatively placed drain should be monitored. This fl uid may be bil-
ious or amylase-rich if a leak is present at the duodenotomy. If unsure, the drained fl uid can
be sent for amylase and bilirubin levels, which should be less than three times the current
serum levels.
◆ Diet can be quickly advanced to normal by 2 to 4 days postoperative.
◆ The drain should not be removed until the patient is tolerating a regular diet. The regular
diet stimulates pancreatic secretion, and duodenal leaks may not be evident until the patient
is tolerating a regular diet.
STEP 5: PEARLS AND PITFALLS
◆ It is helpful to place a biliary balloon catheter through the CBD and into the duodenum
before making your duodenectomy. This is most easily achieved by inserting the catheter
through the cystic duct in a patient who has not had a cholecystectomy, as shown
previously.
◆ If the patient has already had a cholecystectomy, the catheter can be placed through a small
choledochotomy in the CBD.
◆ If gallstones are obstructing the CBD and the catheter cannot be passed, the incision should
be made in the second portion of the duodenum. After the ampulla of Vater is identifi ed,
the incision can be elongated.
Section V • Gallbladder460

◆ The ampulla of Vater can be cannulated retrogradely after the ampulla of Vater is identifi ed,
because it is easier to perform the sphincterotomy over a probe or catheter.
◆ When attempting to cannulate the minor papilla, take great care not to create a hematoma. If
a hematoma forms it may be impossible to cannulate the pancreatic duct at the minor papilla.
SELECTED REFERENCES
1. Mulholland MW, Lillemoe KD, Doherty GM, et al (eds): Greenfi eld’s Surgery: Scientifi c Principles and
Practice, 4th ed. Philadelphia, Lippincott Williams & Wilkins, 2005.
2. Zuidema GD, Yeo CJ, Turcotte J (eds): Shackelford’s Surgery of the Alimentary Tract, 5th ed. Philadelphia,
Saunders, 2002.
3. Cameron JL (ed): Atlas of Surgery: Gallbladder and Biliary Tract, the Liver, Portasystemic Shunts, the
Pancreas, vol 1. Philadelphia, BC Decker, 1990.
4. Cameron JL (ed): Current Surgical Therapy, 8th ed. Philadelphia, Mosby, 2002.
CHAPTER 43 • Sphincteroplasty 461

464
STEP 1: SURGICAL ANATOMY
◆ The liver is suspended in the right upper quadrant by avascular ligamentous attachments.
The falciform ligament is oriented vertically and suspends the liver from the anterior
abdominal wall at its inferior limit to the diaphragm just anterior to the vena cava. The left
and right triangular ligaments extend in a transverse direction, beginning on the lateral
borders of both the left and right liver, coursing along the diaphragm, and terminating at
the vena cava where they join the superior extent of the falciform ligament. The triangular
ligaments are composed of both anterior and posterior leafl ets.
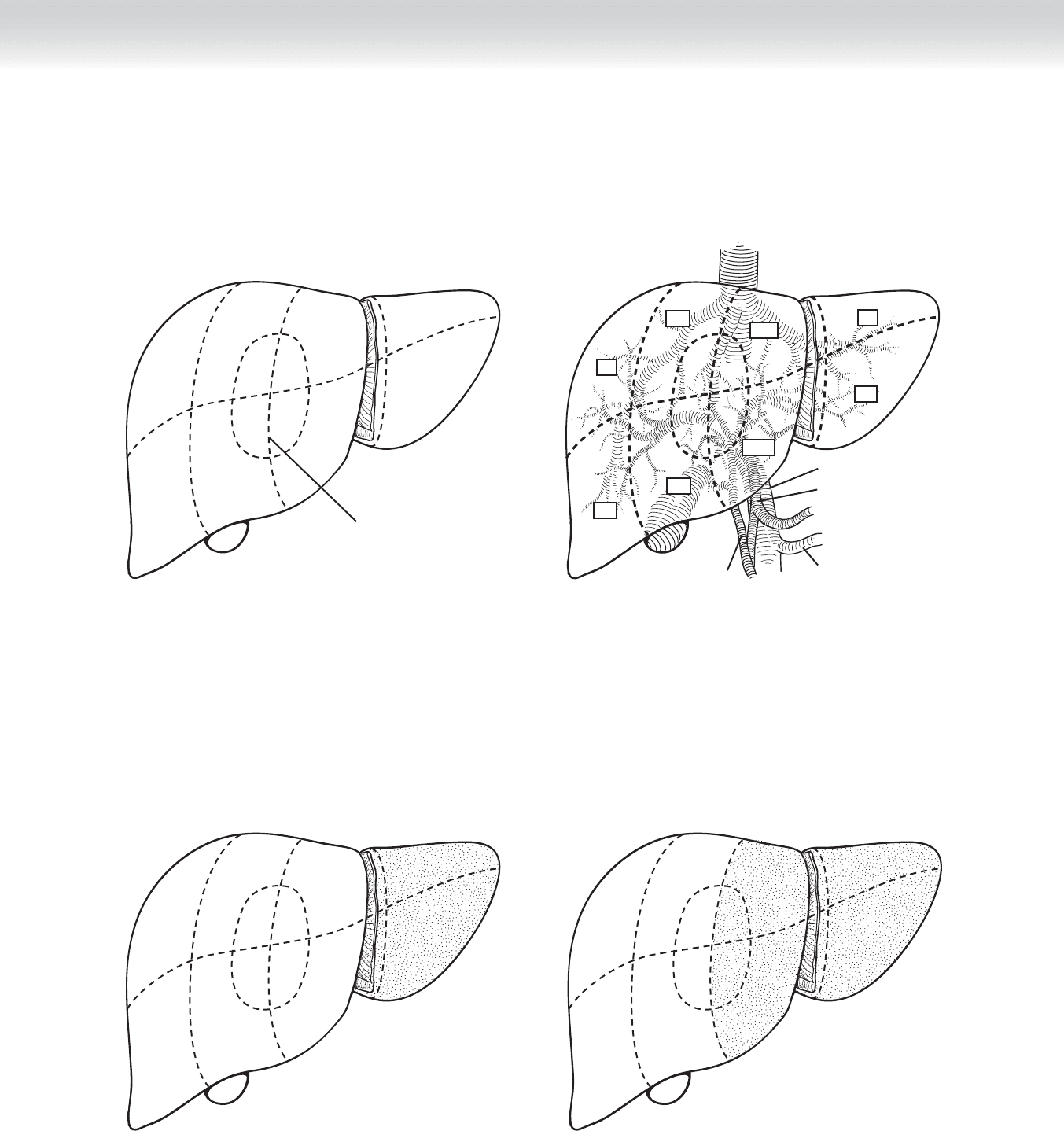
◆ Based on the intraparenchymal anatomy, the liver is divided into left and right livers, each
composed of four segments. The line of demarcation is located several centimeters to the
right of the falciform ligament and projects in a line, which transects the gallbladder bed
from anterior to posterior (Figures 44-1 and 44-2).
◆ On gross examination, the liver appears to be composed of two discrete lobes. Thus, there
is a traditional terminology in which the left and right lobes are defi ned by the falciform
ligament. Resection of one of these is termed a left or right lobectomy. This terminology has
largely been replaced by one based on the intraparenchymal vascular and biliary structures
(Figures 44-3 and 44-4).
◆ The left liver is served by the left portal vein, left hepatic artery, and left bile duct. It is
composed of segments I, II, III, and IV. Segments II and III represent the traditionally
termed left lobe. Segment II is located at the surface of the left hemidiaphragm, and seg-
ment III occupies the inferior aspect of the left lobe. The boundary between the two ex-
tends horizontally approximately midway through the left lobe. Segment I is also called the
caudate lobe. It occupies the posterior aspect of the liver in the midline. The segment wraps
rather like a collar around the vena cava on its left aspect. This segment is unique for its
venous drainage, which is independent of the left or middle hepatic veins and is composed
of multiple tiny tributaries between the vena cava and the segment. Segment IV, termed the
quadrate lobe, occupies the area between the falciform ligament medially and the gallblad-
der bed laterally. It is the only segment that has been designated to have two discrete com-
ponents. IV-A is the anterior half of segment IV, and IV-B is the posterior half. This distinc-
tion can be signifi cant in nonanatomic resections (see Figures 44-1 and 44-2).
CHAPTER
44
Segmental Hepatic Resection—Left
Lateral Segmentectomy
and Nonanatomic Resections
William H. Nealon
CHAPTER 44 • Segmental Hepatic Resection 465
VII
VIII
V
VI
IV-B
IV-A
II
III
Hepatic Segments
Cantlie’s line
FIGURE 44–1
I
Common bile duct
Hepatic artery
Splenic vein
Portal vein
V
VI
IV-B
III
VII
VIII
IV-A
II
FIGURE 44–2
VII
VIII
V
VI
IV-B
IV-A
I
II
III
Left Lobectomy
FIGURE 44–3
VII
VIII
V
VI
IV-B
IV-A
I
II
III
Left Hepatectomy
FIGURE 44–4
466 Section VI • Liver
◆ The right liver is composed of segments V, VI, VII, and VIII. These four are oriented around
a horizontal line transecting the right liver at its mid-portion and similarly by a vertical line,
which transects the right liver at its mid-portion. Beginning at the inferomedial segment V,
the segments follow a clockwise direction, with VI inferolateral, VII superolateral, and VIII
superomedial (see Figures 44-1 and 44-2).
◆ Lymphovascular and biliary structures exit the liver through the hepatoduodenal ligament,
which courses between the duodenum into the base of segments IV and V—an area that is
termed the porta hepatis. The portal triad of microanatomy is matched by the gross ana-
tomic orientation in the hepatoduodenal ligament, composed of hepatic artery, portal vein,
and bile duct. Each structure divides into a left and right branch and then arborizes within
the liver in a pattern defi ned by the segments (see Figures 44-1 and 44-2).
◆ Venous drainage of the liver is primarily located at the superior aspect of the liver in the
midline in short structures between the vena cava and the liver. The left, middle, and right
hepatic veins each enter the vena cava within 2 to 4 cm of one another in a coronal orien-
tation. One or all of these venous elements may be intrahepatic or may have exceedingly
short extrahepatic components. This anatomic feature raises considerably the risk of uncon-
trolled hemorrhage during dissection and resection (see Figure 44-2). In addition to these
three venous structures, there are between 2 and 20 tiny tributaries between the posterior
surface of the liver and the contiguous vena cava. These must be divided to fully mobilize
the right liver.
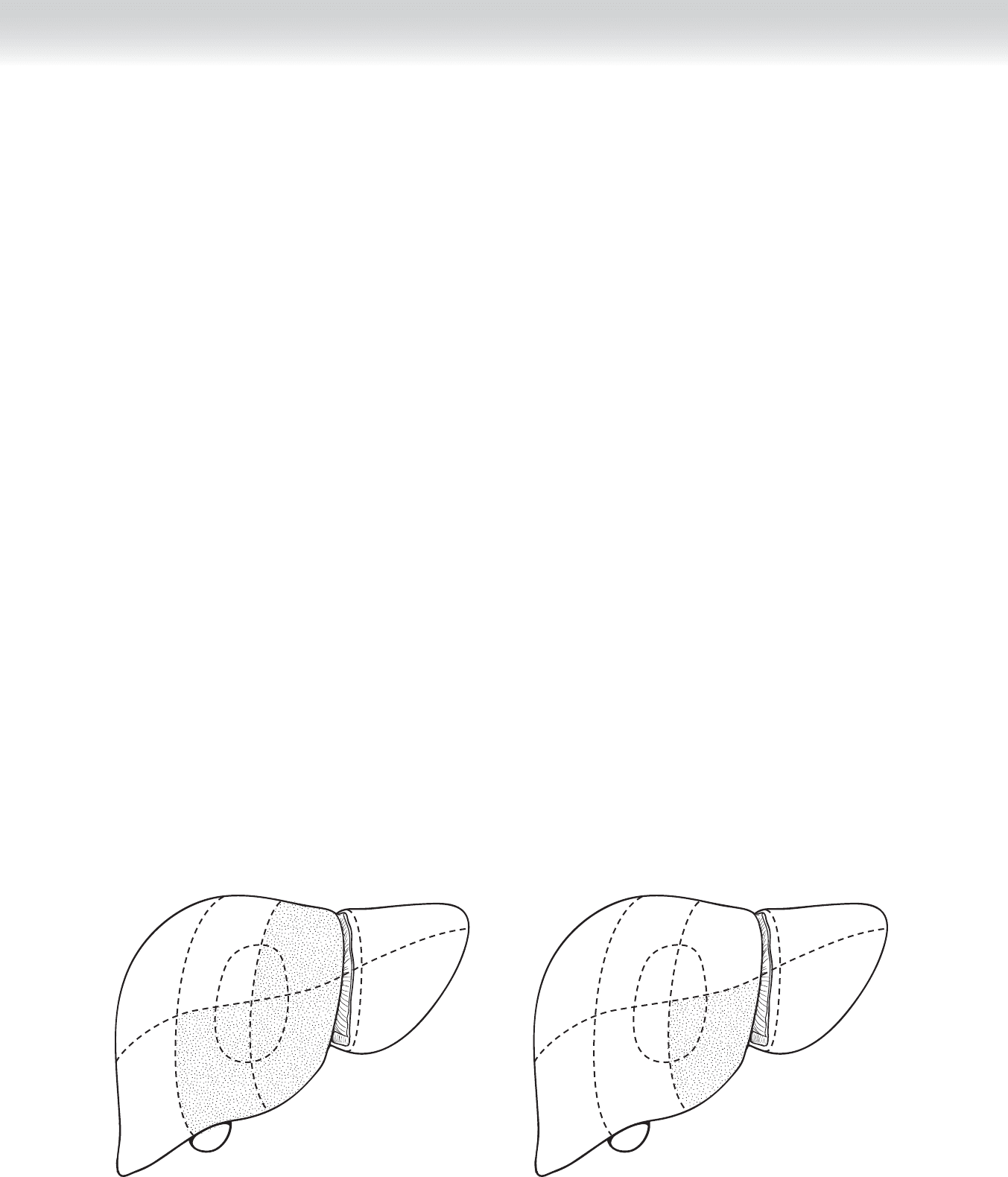
◆ In discussions of nonanatomic resections, one must recognize that similar principles will
be used for essentially all such procedures, and there are a wide variety of examples. In
patients with gallbladder cancer, for example, one may choose to perform a complete resec-
tion of the gallbladder bed by performing a segment IV, V resection (Figure 44-5), or one
may choose to perform an isolated segment IV-B resection (Figure 44-6).
VII
VIII
V
VI
IV-B
IV-A
I
II
III
Resection of Segments IV and V
FIGURE 44 –5
VII
VIII
V
VI
IV-B
IV-A
I
II
III
Resection of Segment IV-B
FIGURE 44 –6

CHAPTER 44 • Segmental Hepatic Resection 467
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Due to the magnitude of hepatic surgery, one fi rst consideration is the medical status of the
patient and likely risk of surgery. Thus one must exclude signifi cant coronary, pulmonary,
or renal disease or age and frailty. Of particular concern in relation to hepatic surgery is the
underlying hepatic function. Because hepatocellular carcinoma is associated with prior hep-
atitis and cirrhosis, one must determine fi rst whether cirrhosis exists and second what level
of function is apparent. Historically, this was measured by examining synthetic and excre-
tory functions and measures of portal hypertension (serum albumin level, coagulation pro-
fi le, serum bilirubin level, ascites, and mental status/serum ammonia). More recently, the
Model for End-Stage Liver Disease (MELD) score was developed as a means of segregating
candidates for liver transplant. This system incorporates prior variables, but has added and
places considerable signifi cance to renal function. Particularly when one anticipates a major
resection, one must establish that suffi cient liver will remain to support life. Unfortunately,
this estimate of “hepatic reserve” is even today an inexact science.
◆ Nutritional status, renal function, degree of ascites, and coagulation abnormalities are all
factors that may be improved by medical management before surgery. Unfortunately, we have
personal experience that such patients may thereby achieve an improved functional grade
but appear to carry a risk that exceeds the risk in patients who have had this improved func-
tional status without a need for medical manipulation to achieve it.
◆ In the case of malignancy, one must establish that curative resection is clinically achievable.
STEP 3: OPERATIVE STEPS
1. INCISION
◆ We prefer the inverted L incision.This incision offers the option of extending the horizontal
component of the incision either laterally into the right fl ank or medially across the mid-
line. The vertical component of the incision can be extended toward the xiphoid process.
By then placing self-retaining retractors, the exposure of the right upper abdomen is maxi-
mized. The incision can be extended if the operative view is inadequate.
2. DISSECTION
◆ First, the concept of nonanatomic resections encompasses wedge resections, which do not
require individual segmental dissection. The term also encompasses the many variations on
segmental or multisegmental resections.
◆ For wedge resection, most surgeons will use a combination of total infl ow occlusion with
compression of the hepatoduodenal ligament combined with local compression at the site
of resection.

468 Section VI • Liver
◆ For segmental resection, although a vast variety of procedures are included in this category,
the concept is the same. Vascular control is obtained by dissecting along the hepatoduode-
nal ligament and accessing and temporarily or permanently occluding the vessels corre-
sponding to that segment or the primary feeding vessel to that segment. To illustrate, we
will describe the steps involved in resection of segment VIII (Figure 44-7).
◆ Inferior to the liver edge, divide the falciform ligament between clamps and tie with heavy
silk suture. Cut the sutures at the caudal divided ligament. Place a hemostat on the uncut
cephalad end of suture on the divided ligament for use in manipulating the liver during dis-
section. You will discover the need for a constant balance between retracting the liver ceph-
alad and retracting caudad. Using this tether, you may restore some caudal exposure while
the self-retaining retractor suspends the liver toward the diaphragm (Figure 44-8).
◆ Using electrocautery, the fi lmy, avascular falciform ligament is incised beginning at its attach-
ment to the anterior abdominal wall and continuing in a cephalad and dorsal direction up to
the point of convergence of this ligament with the left and right triangular ligaments. The
hepatic veins are visualized at the superior extent of this dissection. Carefully incise the peri-
toneal surface to clearly defi ne the right and middle hepatic veins. We favor placing a vessel
loop around the right and middle hepatic veins at this juncture.
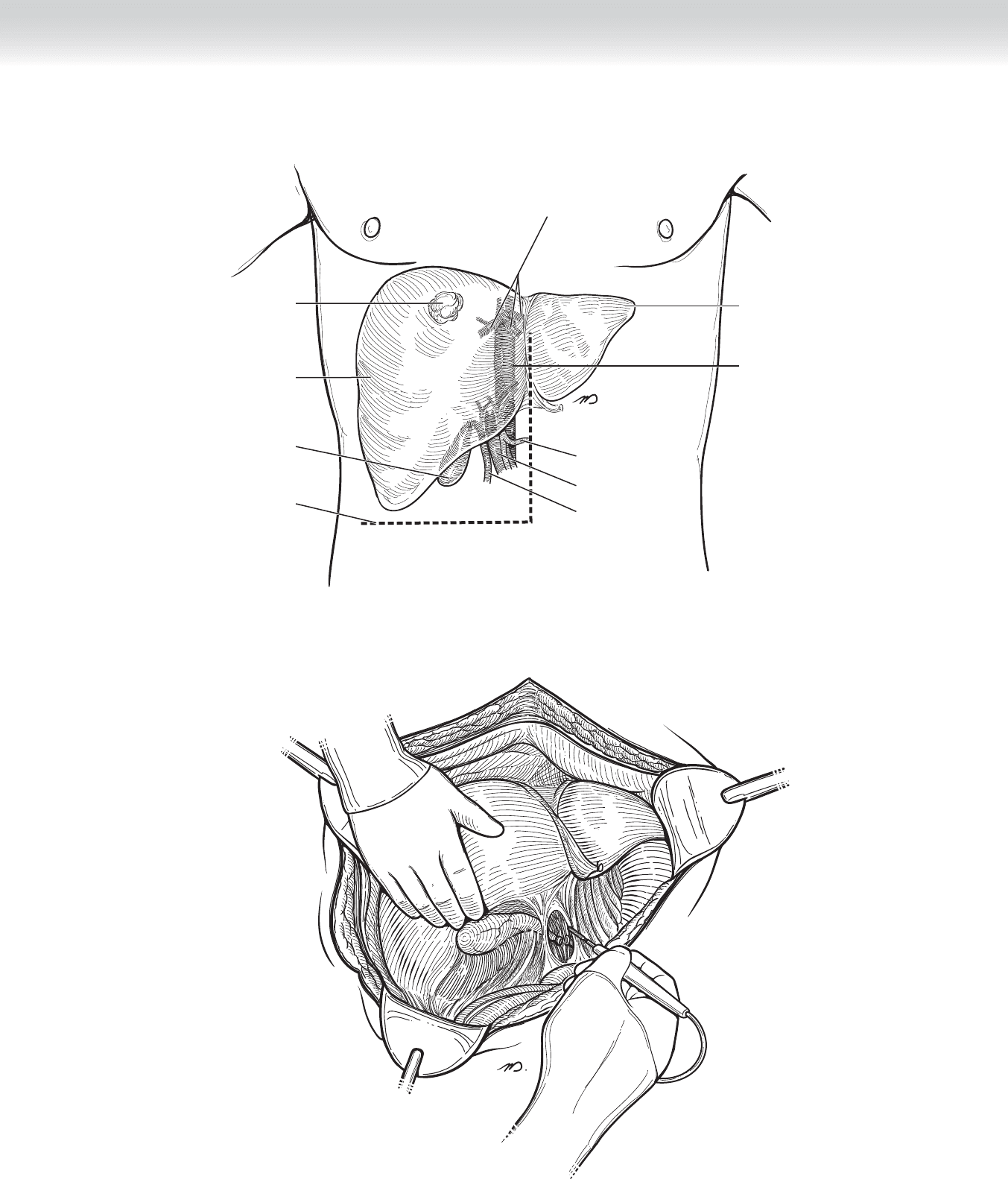
CHAPTER 44 • Segmental Hepatic Resection 469
Inferior vena cava
Hepatic veins
Gallbladder
Incision
Lesion
Left lobe
Right lobe
Common
hepatic artery
Portal vein
Common bile duct
FIGURE 44 –7
FIGURE 44 –8

470 Section VI • Liver
◆ Divide the anterior and posterior leafl ets of the right triangular ligament using electrocautery.
It is usually best to fi rst extend the incision of the anterior leafl et from the right lateral margin
to the midline. At this point, gentle blunt dissection will separate the diaphragmatic attach-
ments, better revealing the posterior leafl et and facilitating division of this structure. In this
fashion, the liver is mobilized to the midline, as well as in a caudal direction (Figure 44-9).
With full mobilization, it is possible to bring the liver into the midline, affording a wide access
to the entire liver.
◆ Dissect the peritoneum overlying the hepatoduodenal ligament in a transverse direction.
After dividing the typically fi lmy gastrohepatic or lesser omentum medial to the ligament, it
is possible to pass your fi nger or an instrument into the foramen of Winslow and completely
encircle the structures contained in the hepatoduodenal ligament. Pass an umbilical tape
around the ligament, and using the hooked instrument with a section of rubber tubing create
a Rummel loop. This safety measure is performed to permit complete infl ow occlusion
should this be necessary to control undue hemorrhage if encountered at any time during the
procedure. Place a hemostat on the two loose ends of umbilical tape (Figure 44-10).
◆ At approximately the mid-portion of the hepatoduodenal ligament, dissect and isolate the
common bile duct laterally and the proper hepatic artery located on the medial edge of the
ligament. Place a
1
⁄4-inch Penrose drain around the bile duct and a vessel loop around the
artery, and use traction on these two structures to reveal the portal vein positioned between
and posterior to these two parallel structures. Gently tease the fi lmy adhesions to isolate all
three structures and extend this dissection toward the hilum.
◆ Follow the common bile duct, hepatic artery, and portal vein toward the hilum of the liver,
and then isolate and encircle the right branch of each structure. Each of these will follow a
course directed toward the gallbladder bed, which rises at approximately a 60-degree angle
from the hilum toward the right liver.
◆ Interrupt vascular infl ow to the right liver temporarily by placing atraumatic vascular
clamps on the right hepatic artery and right portal vein.
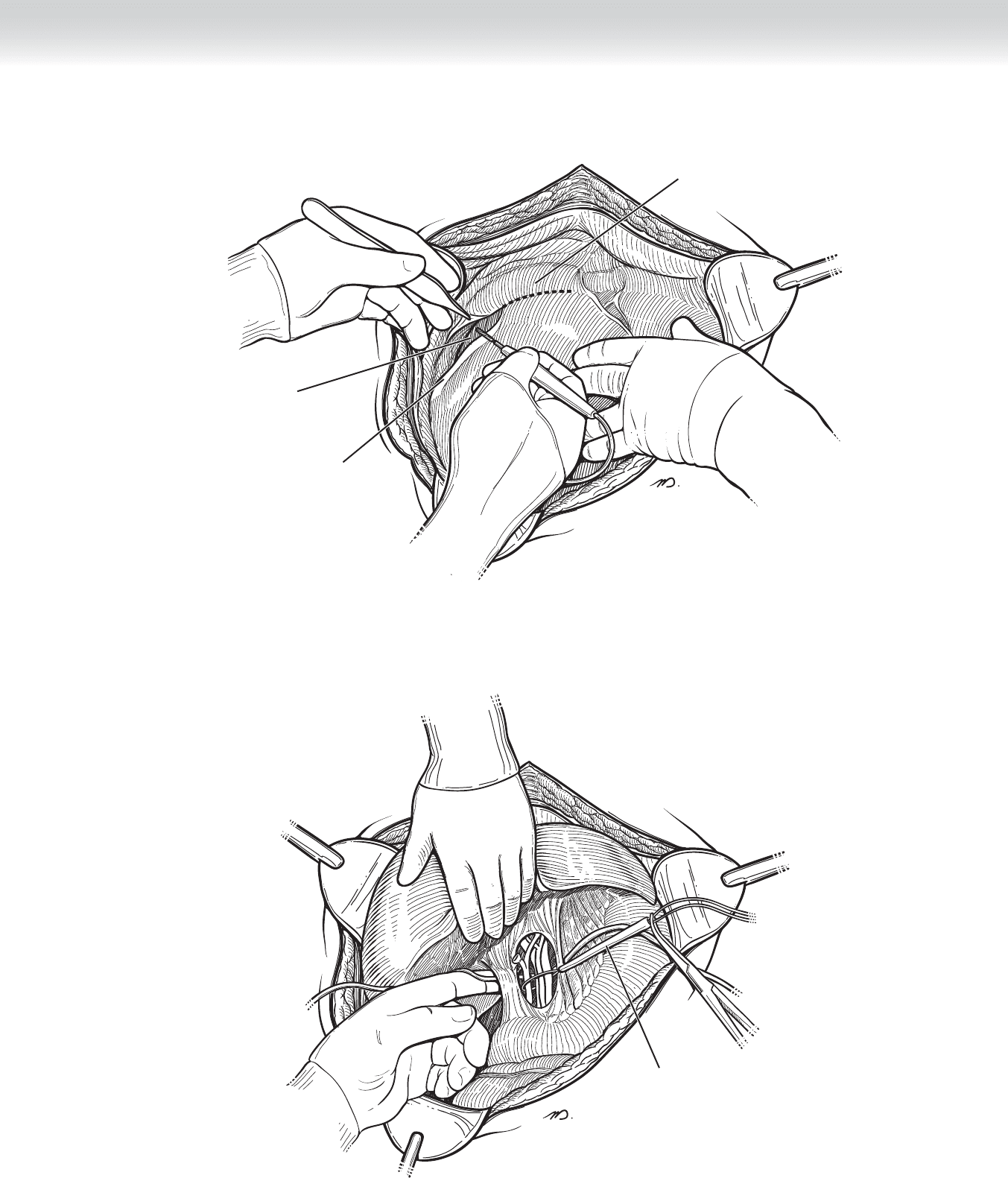
CHAPTER 44 • Segmental Hepatic Resection 471
Right triangular
ligament
Diaphragm
Bare area
FIGURE 44 –9
Rummel loop
(inflow occlusion)
FIGURE 44 –10