Yam, Kit L. (ed.). The Wiley encyclopedia of packaging technology
Подождите немного. Документ загружается.


propose modifying the well-known engineering design
process as follows:
1. Define the objectives and scope for the materials-
handling system.
2. Analyze the requirements for handling, storing, and
controlling material.
3. Generate alternative designs for meeting materials-
handling system requirements.
4. Evaluate alternative materials-handling system
designs.
5. Select the preferred design for handling, storing,
and controlling material.
6. Implement the preferred design, including the selec-
tion of supplies, training of personnel, installation,
debug and startup of equipment, and periodic audits
of system performance.
Several other authorities in the field also suggest using
this approach. Utilizing the expanded list of objectives and
the principles of materials handling serves to address step
1 of this process. The next four steps can be approached
qualitatively, or quantitatively. A qualitative analysis may
take a questioning approach with yes/no or scaled/
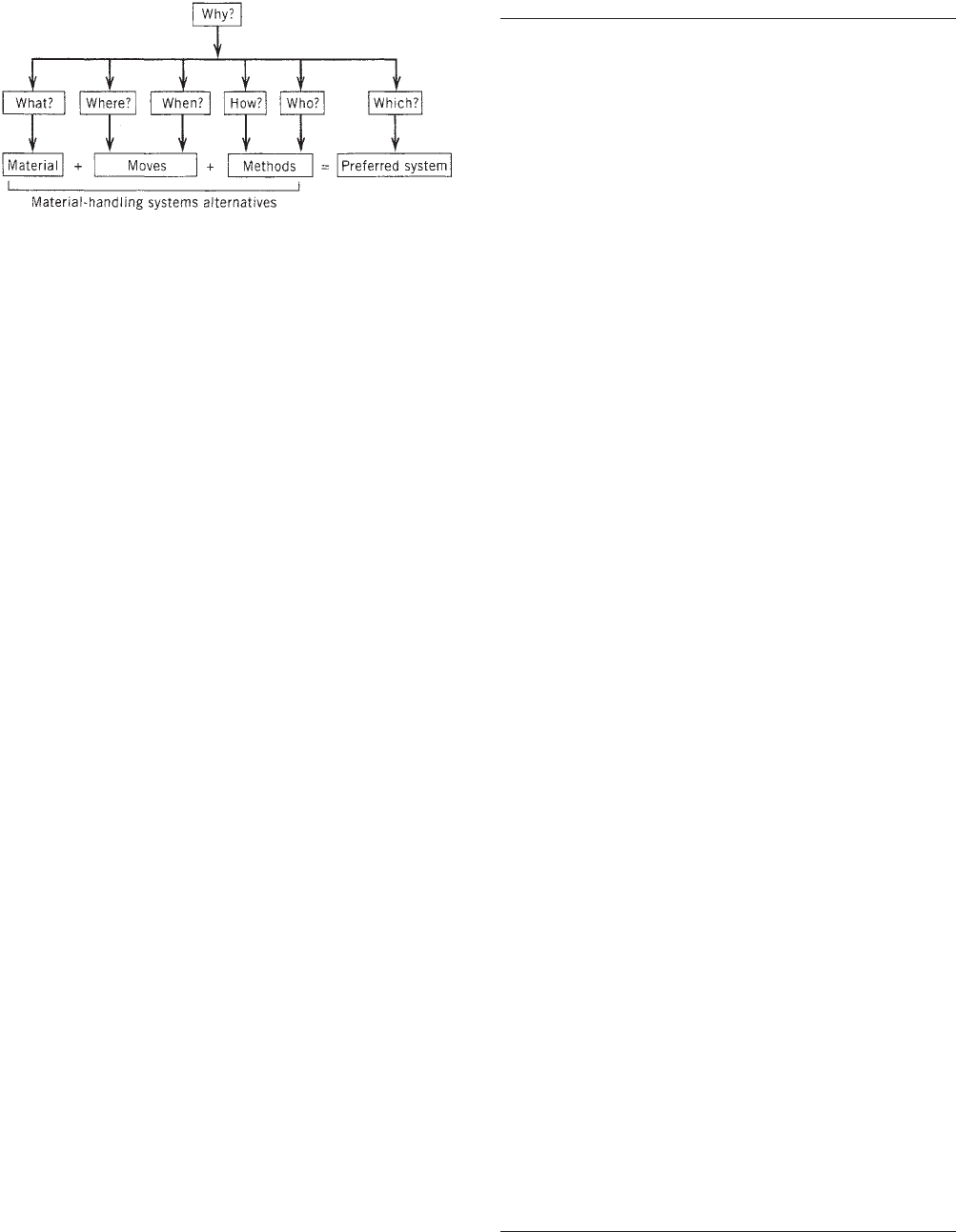
weighted answers. Basic questions to consider asking
when addressing the system under study include ‘‘why,’’
‘‘what,’’ ‘‘where,’’ ‘‘when,’’ ‘‘how,’’ and ‘‘who,’’ and ‘‘which.’’
More specifically, and at a minimum, Tompkins and White
suggest asking and answering a set of questions as shown
in Table 2 (see also Figure 1).
This ‘‘questioning attitude’’ leads to the basic equation
of developing the best materials, moves, and methods to
arrive at the preferred system. Some issues to consider in
this equation include the type of materials and their
physical characteristics, the quantities of the materials
to be moved, frequency of moves, sources of moves, and
methods by which this may occur.
Numerous checklists are available in the literature
that aid in qualitative analysis and help to answer the
basic questions listed above (2, 4–6). It should be noted
that any checklist may have to undergo a certain amount
of modification to fit the system at hand. Certain aspects of
the checklist may not be appropriate, or additional aspects
may be required. However, the previous stated objectives
as well as the principles of materials handling can facil-
itate selection or development of checklists for use as a
qualitative analysis tool. One such example of a recent
checklist as compiled by Gelders and Pintelon (2) is shown
in Table 3.
Quantitative analysis can provide an objective basis to
evaluate MHSs as compared with the more subjective
qualitative techniques. This may include computing mea-
sures such as efficiency, which can be defined as the
theoretical computed input divided by the actual con-
sumed output; effectiveness, which is the actual achieved
output divided by the theoretical expected output; and
productivity, which is defined as output over inputs.
Gelders and Pintelon (2), among others, refer to these as
performance indicators (a related discussion of these
issues can be found in the article by Zepf in this
Encyclopedia). For instance, throughput time (cycle
time) is one measure of effectiveness, use of warehouse
space, or pallet space (unit load) is a measure of efficiency,
and productivity may be measured in terms of labor
Table 2. Basic Materials-Handling System Design
Questions
Why
Is handling required?
Are the operations to be performed as they are?
Are the operations to be performed in the given sequence?
Is material received as it is?
What
Is to be moved?
Data are available and required?
Alternatives are available?
Are the benefits and disbenefits (costs) for each alternative?
Is the planning horizon for the system?
Should be mechanized or automated?
Should be done manually?
Shouldn’t be done at all?
Other firms have related problems?
Criteria will be used to evaluate alternative designs?
Exceptions can be anticipated?
Where
Is materials handling required?
Do materials-handling problems exist?
Should materials-handling equipment be used?
Should materials-handling responsibility exist in the
organization?
Will future changes occur?
Can operations be eliminated, combined, or simplified?
Can assistance be obtained?
Should material be stored?
When
Should material be moved?
Should I automate?
Should I consolidate?
Should I eliminate?
Should I expand?
Should I consult vendors?
Should a postaudit of the system be performed?
How
Should materials be moved?
Do I analyze the materials-handling problem?
Do I sell everyone involved?
Do I learn more about materials handling?
Do I choose from among the alternatives available?
Do I measure materials-handling performance?
Should exceptions be accommodated?
Who
Should be handling materials?
Should be involved in designing the system?
Should be involved in evaluating the system?
Should be involved in installing the system?
Should be involved in auditing the system?
Has faced a similar problem in the past?
Which
Operations are necessary?
Problems should be studied first?
Type equipment (if any) should be considered?
Materials should have real-time control?
Alternative is preferred?
Source: Reprinted with permission from Tompkins and White (5).
708 MATERIALS HANDLING
components relative to the materials-handling function.
Comparing these or other measures against predefined
targets may help to direct modifications to the entire
MHS, or only portions of the same.
Overall MHS analysis may be accomplished through
the use of simulation software. The software can be used
to compare various alternatives against specified criteria
and to perform what-if analysis (7–9). Most current simu-
lation software packages offer animation capabilities that
allow the designer to see dynamic representations of the
system under study. Specialized software such as CAPE
(10) or TOPS (11) may be used to focus on palletization and
the unit-load concept as well as optimized package design.
Simple spreadsheet analysis that uses macro program-
ming may also be used for this purpose. Beyond ones own
operations, benchmarking, that is, comparing one’s own
strengths and weaknesses to a competitor, may also be
applied relative to materials-handling analysis.
One of the earlier structured approaches to MHS
analysis was developed by Muther and Haganas (12).
Their method, systematic handling analysis (SHA), was
developed from the premise that any analysis must de-
pend on material, moves, and methods. They describe the
approach as ‘‘an organized, universally applicable ap-
proach to any materials-handling project,’’ consisting of
a ‘‘framework of phases,’’ ‘‘pattern of procedures,’’ and ‘‘set
of conventions.’’ They further identify four phases as
‘‘external integration,’’ ‘‘overall handling plan,’’ ‘‘detailed
handling plan,’’ and ‘‘installation.’’ The total methodology
makes extensive use of charts, checksheets, flow charts,
and detailed procedures. In short, the method provides a
systematic approach to determine solutions to materials-
handling problems. When used in conjunction with the
basic principles of material handling, it can provide a
powerful framework for identifying good solutions to
material handling problems.
PLANT LAYOUT AND FACILITIES LAYOUT
Materials handling is an integral part of plant layout.
Conversely stated, plant layout is an integral part of
materials handling (the proverbial chicken and egg). In
short, both MHS design and plant layout design must go
hand-in-hand. A cursory review of the stated objectives of
materials handling and the MHS principles reveals
Table 3. Checklist for MHS
General questions
Topic: Global aspects of the MHS
Examples: Is the MHS flexible enough to cope with changing
product volumes and mixes, throughput and service needs,
technology options, customer requirements, etc.?
Is the MHS integrated with the production system? Are
interfaces with other business functions working okay?
Is standardization a main concern while investing in new
equipment?
Has the company clear objectives concerning the degree of
automation to apply to the MHS?
Specific questions
Topic: Different areas of (and interfaces with) the MHS
Examples:
Receiving, including dock operations and inspection
Does the dock equipment match the types of warehouse
help to reduce energy costs?
Could doors between dock and warehouse help to reduce
energy costs?
Do quality control and inspection reports satisfy the needs
of the customer, i.e., the manufacturing process?
Storage
Are there any unnecessary packing-unpacking operations
needed because of a lack of standardization or choice of the
wrong unit load?
Is the storage equipment sized correctly for the material
stored?
Is the tradeoff between storage density and selectivity
optimized?
Handling operations in the manufacturing process
Is there any backtracking in the flow path?
Are there any areas with traffic congestion?
Is production work delayed because of poorly scheduled
delivery and removal of material?
Other picking
Are travel distances between picks minimized where
possible?
Would a part-to-picker instead of a picker to part system
improve the picking operations?
Are low-activity items out of the way but accessible to
pickers when necessary?
Packaging
Are mispicked orders corrected in a timely manner?
Is volume sufficiently high to justify addition of automatic
packing equipment to replace manual operations?
Did you make the right choice between strapping,
wrapping, etc.?
Shipping
Are receiving and shipping operations separated so that
they do not interfere?
Are the shipping operations well planned?
Would additional equipment speed up the loading
operations?
Information flow and data collection
Topic: The amount and type of data collected, the data
processing, and information flow accompanying the material
flow
Examples:
Does a computerized database of inventory information
exist?
Does each stockkeeping unit have a unique identification
number?
Is there a satisfactory performance reporting?
Source: Reprinted with permission from Gelders and Pintelton (2).
Figure 1. Basic equation for materials-handling system design.
Reprinted with permission from Tompkins and White (5).
MATERIALS HANDLING 709
commonalties, for instance, increase space and equipment
use and improve safety and working conditions (objec-
tives), flow, utilization, and space use (principles). These
objectives and principles, to name just a few, are also
pertinent to effective facilities and plant layout.
Facilities layout, much like material handling, is a
volumous subject in and of itself. However, for the pur-
poses of this chapter, some methods of analysis are briefly
discussed. The techniques used may be simple or complex,
and either quantitative or nonquantitative. Tompkins
and White (5) provide a comprehensive discussion of the
subject matter. The most basic method to determine
layout design is by way of scaled templates of the facility,
machinery, material, and people. The templates can be
arranged using heuristics to determine the most appro-
priate layout. This can be accomplished with the aid of
computer-aided-design (CAD) packages. When areas of a
facility can be departmentalized, matrix techniques
such as from–to charts, or ‘‘closeness’’ charts may be
used. If some objective such as minimizing materials-
handling costs, or minimizing distances traveled can be
identified, several optimization models may be used (13).
A complete methodology, systematic layout planning
(SLP), developed by Richard Muther, and similar in
nature to systematic handling analysis (SHA) also is
effective for use in existing or new facilities. Similar to
SHA, it consists of a framework of phases, a pattern of
procedures, and a set of conventions. In general the
process includes four overall phases of establishing a
location, planning the general overall layout, preparing
detailed layout plans, and finally installation at the facil-
ity. Also like SHA, the method is logical in nature, includes
detailed graphic procedures, and leads to good solutions
based on the initial inputs.
Numerous computer software programs have been
developed which address facilities layout. Three such
programs are ALDEP (automated layout design program),
CORELAP (computerized relationship layout planning),
and CRAFT (computerized relative allocation of facilities
technique) (13). More recently, factory CAD, factory plan,
and facility plan flow suite of facilities-planning software
(14) has been introduced based largely on the procedures
pioneered by Muther. Programs such as these are useful
when problems are large and complex. However, they are
not guaranteed to provide optimum solutions. Experience,
judgment, and intuition are still necessary when using
this or other kinds of software.
MATERIALS-HANDLING EQUIPMENT, MATERIAL, AND
METHODS
An abundance of materials-handling equipment exists for
various applications. Usually, there are multiple choices
for each application. The literature for materials handling
contains guidelines, tables, and classification schemes to
help in selecting the right equipment for the right purpose
(1, 3). Furthermore, the proper use of the principles of
materials handling and appropriate checklists, in line
with stated objectives, can also serve to identify the right
equipment for the given application. In general, the three
broad categories of materials-handling equipment are
trucks, conveyors, and cranes and hoists. In the total
systems concept, storage devices such as pallet racks
and bins, automated storage, and retrieval systems are
also included; pallets, slipsheets, and returnable contain-
ers are examples of material and methods.
MATERIALS HANDLING AND PACKAGING
The previous sections of this article discussed general
principles, objectives, and techniques of materials hand-
ling in a broad sense without reference to a particular
industry or manufacturing application. However, as the
most comprehensive definition (6) stated earlier implies,
the issue of material handling is usually not singular in
nature but is indicative of a more complex and compre-
hensive system. Consequently, materials handling can be
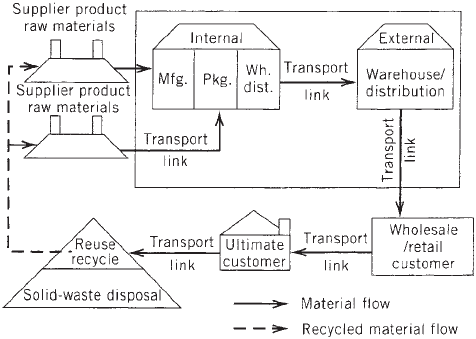
approached from a systems perspective. Figure 2 illus-
trates the extent to which a systems view can be taken.
This view shows an inclusive life-cycle approach that
includes the supplier of the basic raw material and
extends to disposal of the product and package. Decision-
making criteria related to material handling, therefore,
should extend beyond the confines of the ‘‘manufacturing’’
facility, or process, to include issues related to packaging,
distribution and warehousing, wholesale or retail, the
consumer, and solid waste.
Packaging, like materials handling, can also be viewed
from a systems approach as shown in Figures 3 and 4.
Figure 3 shows the broad, interdisciplinary nature of
packaging, and identifies the functions it must address,
ie, containment, protection, communication, and perfor-
mance. It also illustrates that a package can be primary,
secondary, tertiary, or quaternary in form and function.
This view also indicates packaging extends beyond the
confines of the ‘‘manufacturing’’ facility, and that a life-
cycle approach toward the development of packaging is
appropriate. The complexity of the systems view is influ-
enced by the product itself and the particular industry
classification. For instance, a consumer foods or
Figure 2. Materials handling in a system context.
710 MATERIALS HANDLING
pharmaceuticals company would have a complex system
that may need to take into account product requirements,
manufacturing requirements, distribution and warehous-
ing requirements, marketing and consumer requirements,
and solid-waste requirements relative to packaging devel-
opment. The range of packaging material, processes, and
equipment in this instance could be wide. However, the
packaging for the manufacturer of a small electric motor
for use in another product may be limited to corrugated
boxes that are hand-packed and hand-palletized.
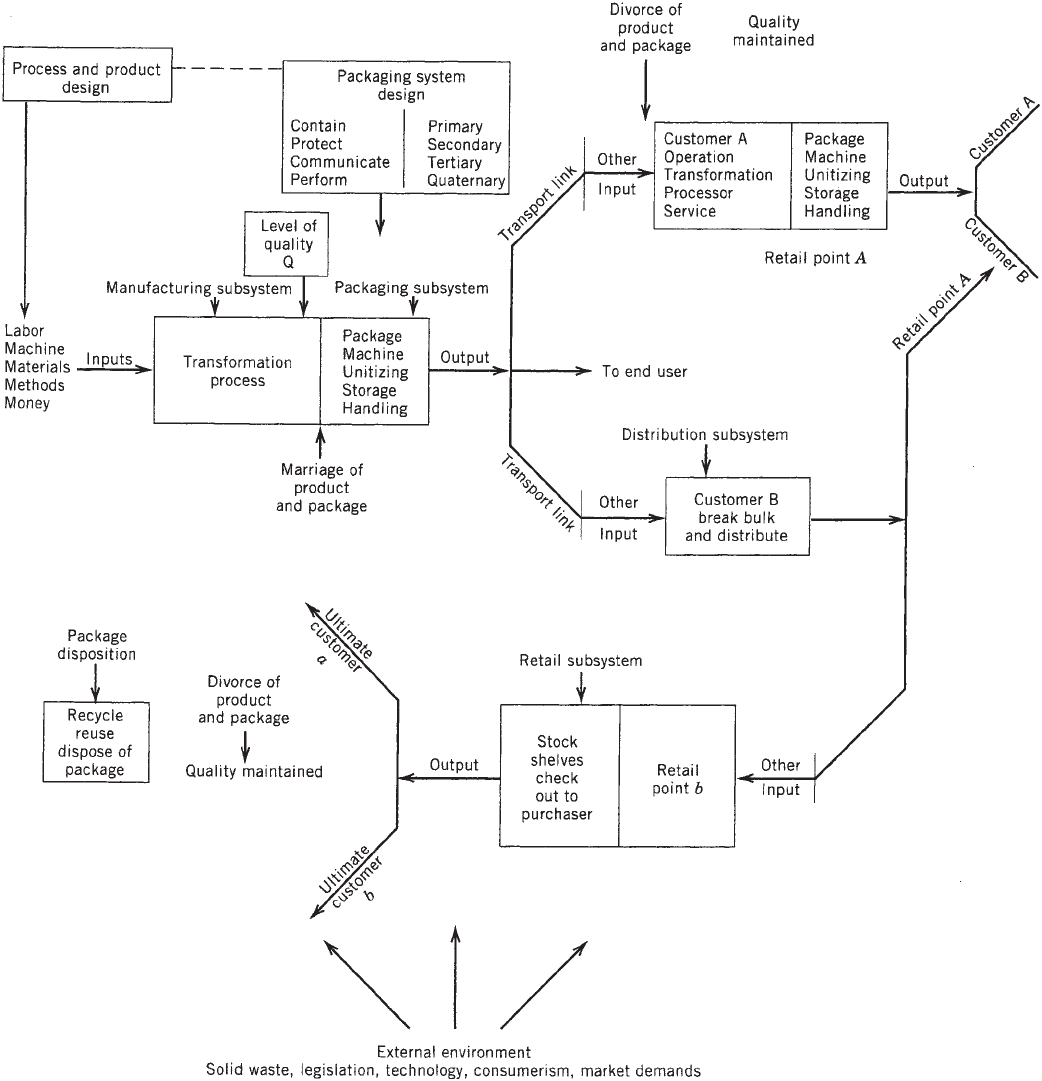
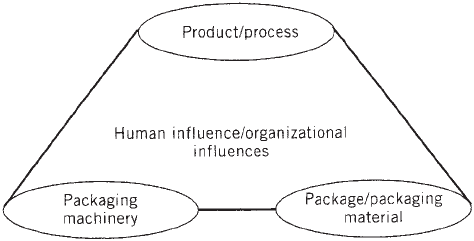
Figure 4 focuses more specifically on the point where
the product, the package, and the package machinery
meet and are united, influenced by human factors (labor
and management policies). This view is relevant at the
initial ‘‘marriage’’ between the product and the primary
package as well as subsequent ‘‘marriages’’ when the
Figure 3. A systems representation of packaging.
MATERIALS HANDLING 711
primary filled package (becomes product) is united to a
secondary package, and so on. This view is typically
confined to the ‘‘manufacturing packaging’’ facility, and
it does not usually extend beyond those boundaries.
Although it is beyond the scope of this article to identify
every packaging issue that influences materials-handling
design, or vice versa, several examples may show that
synergism does exist between material handling and
packaging. In the systems view of both materials handling
and packaging, the concept of the unit load—handle
products in as large a unit load as possible (principle
number 7)—is relevant to each. As previously mentioned,
specialized software (10, 11) exists that can be used to
optimize unit loading on a pallet, for single and mixed
loads, or for optimized loading in the transport vehicle.
Addressing this concept can help to meet objectives such
as reducing materials-handling costs and packaging ma-
terial costs, and also to increase productivity in manufac-
turing and distribution. In addressing the pallet, choices
exist depending on many factors. Choices can be made
between one-way pallets, or closed-loop pallets made from
wood or plastic, one-way or closed-loop pallets made of
recycled material, slipsheets, or no pallet at all. Those
choices, in turn, impact the handling equipment such
as forklift trucks, automated guided vehicles, and so on.
Warehouse storage options such as rack storage or open-
bay storage may also be of concern. Choices on how to
maintain the optimized unit load may also exist. Current
choices include stretch or shrink film, or spot gluing (15),
strapping, and so on, which in turn influences equipment
options. Using closed-loop pallet systems, pallets made
from recycled material, or no pallet at all help to address
material handling principle 12—ecology—which advo-
cates using equipment and procedures that have no im-
pact on the environment.
In the more restricted view of packaging shown in
Figure 4, the packaging line is the primary issue of focus.
Typically, the packaging line will consist of specific packa-
ging machinery (filling, sealing, and labeling), handling
equipment (conveying, accumulation, etc.), inspecting
equipment, coding equipment, and so on, usually begin-
ning at the depalletizer for empty containers and ending
at the palletizer for filled and ‘‘packaged’’ products. The
level of automation of the packaging line may be manual,
semiautomatic, fully automatic, or a fully computer inte-
grated operation.
The integration of the packaging line from a ‘‘macro’’
level through the proper use and selection of various
materials-handling equipment can help to address objec-
tives such as increasing productivity, increasing space and
equipment use, and ensuring a high level of systems
flexibility, reliability, availability, and maintainability,
among others. For example, the choice of the appropriate
conveying and accumulation equipment becomes extre-
mely important depending on a range of factors specific to
the package or packaging material, the speed of the
packaging lines, how flexible the lines must be, and so
on. For instance, handling requirements for empty
lightweight plastic bottles are different from those for
comparable heavier glass containers (16), thus potentially
influencing productivity and other objectives (see the
Conveyors, accumulation, palletizing, depalletizing arti-
cle). Other examples may include the use of robotic
palletizers (see the Palletizers article) increase the flex-
ibility of the packaging line or the use of vertical versus
horizontal accumulation to optimize space and overall
facilities layout. Objectives can also be influenced at a
‘‘micro’’ level by proper design and selection of infeed
mechanisms (star wheels and worm screw), transfer
points (dead plate and power roll), right angle turns, and
so on.
In short, there is much similarity between a systems
view of materials handling and a systems view of packa-
ging. In designing or evaluating packaging systems, issues
relative to materials handling should be addressed. Cor-
respondingly, when designing materials-handling sys-
tems, the requirements of the packaging system must be
addressed as well. This is particularly true for industries
such as consumer foods and products, pharmaceuticals,
and beer and beverages. This is also true for the suppliers
of packaging materials and equipment.
CONCLUSIONS
Materials handling is more than handling material. It
is, in fact, a complex, multifaceted activity that extends
beyond the boundaries of the ‘‘manufacturing’’ facility.
This article has presented definitions, objectives, check-
lists, questions, and techniques that help to understand
the complexities surrounding materials handling. Simi-
larly, packaging is ‘‘more than just a box.’’ This article
briefly shows that packaging can also be viewed from a
systems perspective and that synergies exist between
material handling and packaging. This article mentioned
only a few examples of the commonalties that exist
between materials handling and packaging, but an entire
article could be devoted to the topic. In conclusion, it is
apparent that optimum design for both can depend in
large part on understanding and analyzing each from a
systems perspective.
BIBLIOGRAPHY
1. T. H. Allegri, Sr., Materials Handling: Principles and Prac-
tice, Van Nostrand Reinhold, New York, 1984.
Figure 4. Marriage of product and package.
712 MATERIALS HANDLING
2. L. F. Gelders and L. M. A. Pintelon, ‘‘Material Handling’’ in R.
C. Dorf and A. Kusiak, eds., Handbook of Design, Manufac-
turing and Automation, Wiley, New York, 1994, Chapter 17.
3. D. R. Sule, Manufacturing Facilities: Location, Planning and
Design, 2nd edition, PWS-Kent Publishing, Boston, MA 1994.
4. F. E. Meyers, Plant Layout and Materials Handling, Regents/
Prentice-Hall, Englewood Cliffs, NJ, 1993.
5. J. A. Tompkins and J. A. White, Facilities Planning, Wiley,
New York, 1984.
6. R. E. Sims, Jr., ‘‘Materials Handling Systems,’’ in G. Salvendy,
ed., Handbook of Industrial Engineering, Wiley, New York,
1982, Chapter 10.3.
7. K. J. Musselman, ‘‘Simulations Spectrum of Power In Manu-
facturing’’ in Proceedings, 1990 IIE Integrated Systems Con-
ference & Society for Integrated Manufacturing Conference,
San Antonio, TX, Oct. 28–31, 1990, pp. 65–70.
8. W. S. Haider and S. Rajan, ‘‘Effective Analysis of Manufactur-
ing Systems Using Appropriate Modeling and Simulation
Tools’’ in Proceedings, 1990 IIE Integrated Systems Confer-
ence & Society for Integrated Manufacturing Conference, San
Antonio, TX, Oct. 28–31, 1990, pp. 94–99.
9. A. M. Law and D. W. Kelton, Simulation Modeling & Analy-
sis, 2nd edition, McGraw-Hill, New York, 1991.
10. CAPE—Computer-Assisted Packaging Evaluation, CAPE
Systems Inc., Plano, TX 75074.
11. TOPS—Total Optimization Packaging Systems, TOPS Engi-
neering Corporation, Plano, TX 75075.
12. R. Muther and K. Haganas, Systematic Handling Analysis,
Management and Industrial Research Publications, Kansas
City, MO, 1975.
13. W. J. Stevenson, Production/Operations Management, 4th
edition, Irwin, Boston, MA 1993.
14. Cimtechnologies Corporation, Factory CAD, Factory Plan &
Factory Flow, Release 3.0 Technical and Reference Manuals,
Ames, IA, 1992.
15. ‘‘Palletizing System Brews up Savings for Miller,’’ Packag.
World, 36 (Dec. 1994).
16. P. Reynolds, ‘‘Empty-Bottle Handling Is No Picnic,’’ Packag.
World 42, 46 (Jan. 1995).
MEDICAL DEVICE PACKAGING
LAURA BIX
JAVIER DE LA FUENTE
School of Packaging,
Michigan State University,
East Lansing, Michigan
INTRODUCTION
Medical devices achieve their therapeutic ends via physi-
cal means, as opposed to metabolic, immunological, or
pharmacological processes. The Global Harmonization
Task Force (GHTF) has proposed the following harmo-
nized definition of a medical device:
Any instrument, apparatus, implement, machine, ap-
pliance, implant in vitro reagent or calibrator, software,
material, or other similar or related article:
a. Intended by the manufacturer to be used, alone or in
combination, for human beings for one or more of the
specific purpose(s) of:
. Diagnosis, prevention, monitoring, treatment, or
alleviation of disease.
. Diagnosis, monitoring, treatment, alleviation of,
or compensation for an injury.
. Investigation, replacement, modification, or sup-
port of the anatomy or of a physiological process.
. Supporting or sustaining life.
. Control of contraception.
. Disinfection of medical devices.
. Providing information for medical or diagnostic
purposes by means of in vitro examination of
specimens derived from the human body, and
b. Which does not achieve its primary intended
action in or on the human body by pharmacological,
immunological, or metabolic means, but which
may be assisted in its intended function by such
means (1).
By definition, devices are involved in many different
aspects of healthcare. As such, devices, their manufac-
turing processes, and the packaging that contains and
protects them are extremely disparate. Complicated
capital equipment, such as MRI tunnels and X-ray ma-
chines, are medical devices, but so are simple, commodity-
like items such as tongue depressors and syringes.
Some are meant for mass markets, others are niche items.
Some are packaged individually; others are packaged
in boxes of 100 s or 1000 s. Some are reprocessed,
others are disposable, and some are used for a lifetime.
Risks associated with device misuse and failures are
equally varied, ranging from inconvenience to patient
death (2).
It is estimated that the medical device and equipment
market will be worth $246 billion by 2011, with a 4.6%
annual growth until that time (3). This is largely driven by
aging populations who frequently engage in active life-
styles, a growing middle class in emerging markets, and
the spread of ‘‘Western diets’’ (4).
A hallmark of the device industry is innovation, which
results in short life cycles for many products. ‘‘Medical
devices undergo constant development based on feedback
from medical practitioners and advances in other sciences
relevant to medical device technology’’ (5). ‘‘With this
constant innovation, the medical device industry spends
heavily on research and development’’ (2); a large portion
of revenues go to R&D streams.
CLASSIFICATION OF MEDICAL DEVICES
The great variation present in the medical device industry
means that devices can be classified in a number of ways.
Devices can be categorized by:
. The risk associated with improper use or a failure
(generally high, moderate, and low).
MEDICAL DEVICE PACKAGING 713
. Conditions of processing (reusable, disposable, capi-
tal equipment, etc.).
. Conditions of the therapy (invasive, noninvasive).
. Conditions of shipping and handling (capital equip-
ment, commodity surgical, etc.).
Because the goal of these therapies is to maximize
efficacy and protect patient safety, the most common
way to classify devices is based on risk. Although the
specific classifications and regulatory requirements vary
from country to country, the intent is the same; risk-based
classifications provide guidance regarding the appropriate
level of manufacturing control and regulatory oversight
required to ensure safe and effective products.
GHTF Classification
GHTF, a voluntary group of representatives made up of
regulators and industry, works to encourage convergence
in the evolution of regulatory systems through the use of
guidance documents that can be adopted globally. Because
regulatory scrutiny frequently employs risk-based classi-
fications, and classifications vary throughout the world,
GHTF has tasked a group to catalyze harmonization of the
classification system.
On July 27, 2006 Study Group 1 (SG1) published its
recommendations for device classification entitled ‘‘Prin-
ciples of Medical Devices Classification’’ (6). This docu-
ment is one of a series that, together, describe a global
regulatory model for medical devices; although, at the
time of writing, classification and other regulatory con-
trols were yet to be harmonized.
The GHTF classification system applies to all medical
devices that are not used for the in vitro examination of
specimens derived from the body, and it is based on risk.
Risk is ‘‘a combination of the probability of occurrence of
harm and the severity of that harm’’ (7). Device risk is a
function of (a) the intended purpose of the device, (b) the
effectiveness of risk management techniques applied dur-
ing design, manufacturing, packaging and use, (c) the
intended user, (d) mode of operation, and (e) the technol-
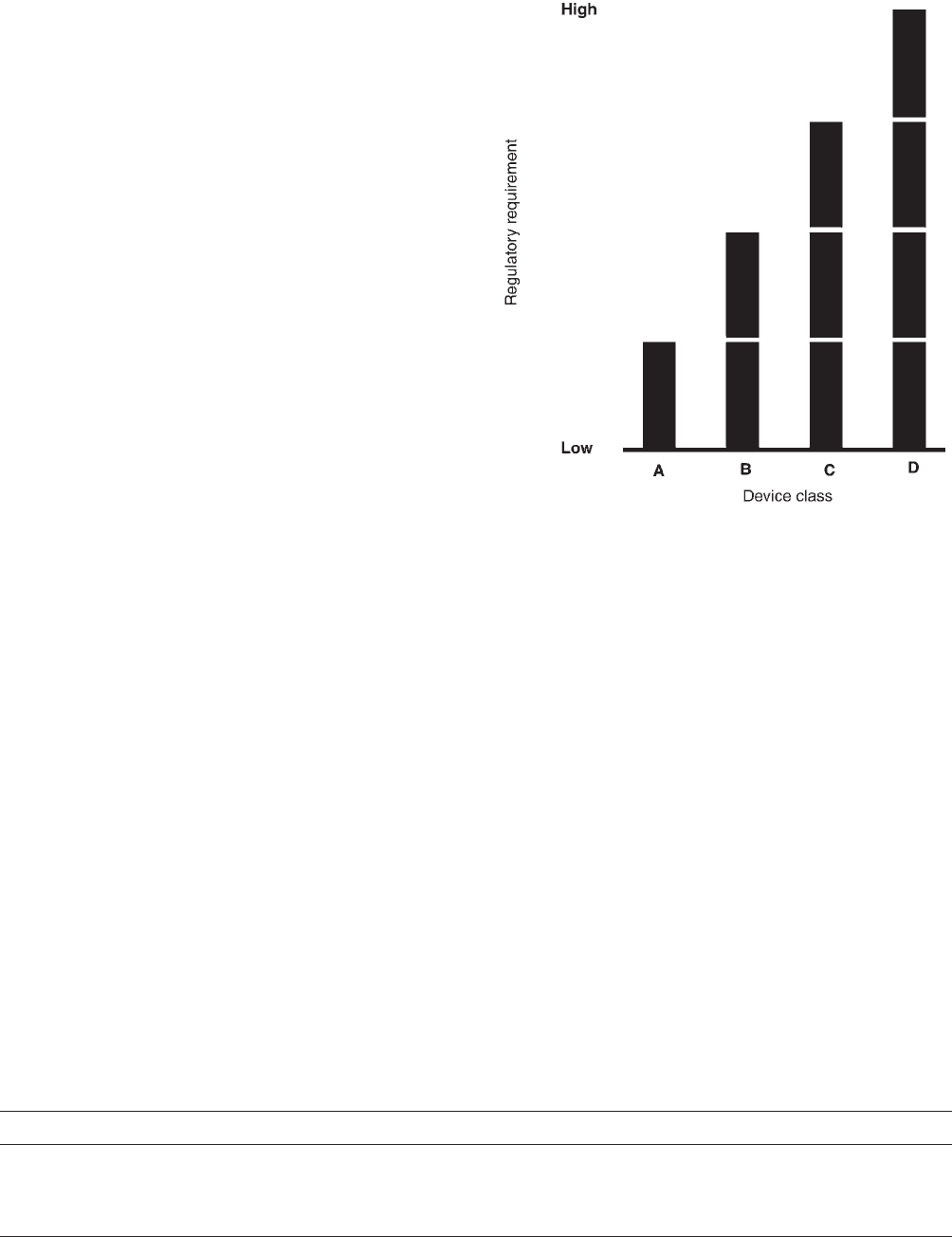
ogy being employed (6). GHTF recommends a classifica-
tion system based on four levels of risk (see Table 1), with
the expected level of control increasing with increasing
risk (see Figure 1). For detailed rules regarding how best
to classify the devices, see ‘‘Principles of Medical Devices
Classification GHTF/SG1.’’
GENERAL CONSIDERATIONS FOR THE DEVELOPMENT
OF MEDICAL DEVICE PACKAGING
Packaging Functions
As a general rule, packaging performs three broad func-
tions—protection, utility, and communication—within
three environments: the physical, ecospheric, and human
(8). (See Packaging Design and Development for more
detail.)
Protection. Protection refers to protection of the medi-
cal device from the environment and vice versa. For
medical device packaging, product protection is necessary
to maintain package integrity throughout its entire life,
including: sterilization, shipping, storage, handling, and
use. Typical issues include protection from shock and
vibration, crushing, puncturing, tearing, bursting, split-
ting, pinholing, humidity, heat, and so on.
Table 1. General Classification System for Medical Devices Proposed by the Global Harmonization Task Group Study
Group 1
Class Risk Level Device Examples
A Low Surgical retractors Tongue depressors
B Low to moderate Hypodermic needles Suction equipment
C Moderate to high Lung ventilators Bone fixation plates
D High Heart valves Implantable defibrillators
Source: Principles of Medical Devices Classification GHTF/SG1/N15.
Figure 1. Relationship of regulatory control and GHTF classifi-
cation. (Source: ‘‘Principles of Medical Devices Classification
GHTF/SG1/N15’’.)
714 MEDICAL DEVICE PACKAGING
The vital importance of maintenance of the sterile
barrier system (SBS) is a distinctive characteristic of
medical device packaging. Medical device packaging for
disposables must not only maintain the SBS but, in many
cases, also facilitate the sterilization of the device within.
Such protective characteristics can be achieved through
the package shape, particularly in thermoformed parts, in
order to avoid product shifting or to keep kit components
separated or nested.
For sealed packages, seal integrity is an important
characteristic in product protection. Seals must be free
of channels and must withstand the rigors of sterilization
and transit.
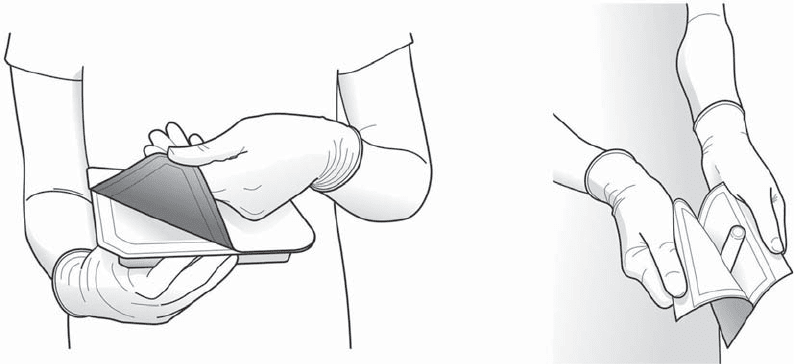
Utility. Utility is related to the ease of use of the
system. For many medical devices, quick and easy opening
and removal of contents are crucial. While this considera-
tion is also important for devices with relatively low risk,
such as an adhesive bandage, it is extremely critical for
sterile medical devices that are used in surgical arenas
where the packaging must allow the device to be removed
without contamination (aseptic presentation; see Figure
2). This particular need has led to the development of
special materials and sealants that, when used in combi-
nation, can provide a package strengths that are adequate
to endure the severity of processing and, at the same time,
can be manually opened without imposing excessive stress
on product or user.
Package design plays a key role in the opening func-
tion. For example, for tray lids, the seal area should
transmit the peeling force smoothly around the package.
The shape of the seal and design and location of the peel
tabs affect the relative ease of opening. Preferably, peeling
tabs are located on the corners of rectangular trays. Lids
should extend slightly over seal areas to avoid edge tear
when peeled. Most designs are based on the classic
‘‘Chevron seal’’ or ‘‘corner peel’’ designs. There are some
cases where the package may serve other functions such
as a measuring device, dispenser, stabilizing stand, dis-
posal receptacle, and other suitable applications (9).
Communication. As with consumer goods packaging,
secondary and primary medical device packages are
a means to convey information through graphics, materi-
als, and shape. Packaging communication operates at
different levels, depending on the type of medical device.
For over-the-counter (OTC) medical devices, such as con-
doms, glucose meters, adhesive bandages, thermometers,
and so on, the communication role involves motivating
a purchase, as well communicating important informa-
tion for the safe and effective use of the medical device.
Information may include directions, warnings, product
benefits, brand differentiation, and so on. A very important
aspect of package communication is product identification.
This is especially true for devices that go into institutional
settings, such as hospitals, where personnel may have
to identify the correct device for a patient when seconds
count.
Increasingly, the manufacturers of medical devices
must provide crucial information in several languages.
The crowded labels can make the legibility, visibility,
and accuracy of the information, all of which are impor-
tant, challenging to achieve. Package manufacturers
not only face these challenges when it comes to labeling
their products, but must also be sure that inks (as well as
other components of the package like adhesives) do
not interfere with the product’s efficacy or safety. In the
event that components of the packaging migrate, it is
important that these unintended additives are nontoxic
and do not degrade or affect the intended performance of
the device.
Package Forms, Materials, and Sealing
Selection of packaging style can impact package integrity.
The type of package is largely driven by the character-
istics of the device being packaged. These include
size, shape, profile, irregularities, density, weight, and
configuration (e.g., single unit or kit). For example, a
high-profile, irregularly shaped device would be more
securely packaged in a semirigid plastic tray than in a
Figure 2. Aseptic presentation.
MEDICAL DEVICE PACKAGING 715
flexible pouch. As such, during the early design stages, it
is critical to define the following parameters:
. Critical product characteristics.
. Type(s) of protection required (physical, ultraviolet
light, O
2
, water vapor transmission, etc).
. Type of sterilization process.
. Where and how the product is going to be dispensed
(OTC, surgery, etc.).
Early packaging forms for medical devices included
bags, cartons, and wraps; the primary material was paper.
Glass and metal containers were used to a lesser extent.
The coming of thermoformable materials in the 1950s and
1960s made tray and blister packaging possible, but the
lack of good lidding materials limited their expansion.
Boxes, cartons, and paper bags were not easy to use,
inconvenient to dispense, and difficult to provide sterile
delivery. The introduction of new thermoplastic polymers
and peelable materials, along with improved film lamina-
tions, has led to the packaging forms most commonly used
today (9). See Table 2 for a summary of materials and
packages of the medical device industry.
Thermoformed Trays. Thermoformed trays are com-
monly used for surgical procedure kits and are ideal for
high-profile, irregularly shaped devices. There are two
types of thermoformed trays: semirigid and flexible. The
most important difference is that semirigid trays are
structurally self-supporting. They can provide good phy-
sical protection and are suitable for multicomponent
applications. Formed flexible packaging is more suitable
for low-cost devices and for simple tray configurations, but
do not offer the same degree of structural protection as the
semirigid trays.
The following characteristics are highly desirable for
all formable materials:
. Ease of forming: The container should be free from
mechanical stress to avoid sterilizer creep or seal
fatigue.
. Heat resistance: The container should withstand
heat sealing without deformation of seal flanges.
. Product compatibility: It is important that packaging
components be nonreactive with the product.
. Sterilization compatibility: The packaging must
withstand the rigors of sterilization and, in many
Table 2. The Relationship Between Materials, Packaging Forms, and Sterilization Methods
Packaging form Sterilization method
Material of the
Sterile Barrier System
(SBS)
Flat pouch
Vented bags
Header bags
Trays
Lids
Gas
Radiation
Steam
Autoclave
Flexible
Paper
Tyvek
®
PET/PE (may be peelable)
PET/PP
Nylon/Sealant
PET or Nylon/Aluminum foil/Sealant
Metallized PET/Sealant
PE (various densities)
Source: Adapted from Berger and Dodrill.
Rigid
PS
PVC
CPET or APET
PETG
PC
XT polymer
Polyacrylonitrile
HDPE
PP
CTFE (Aclar
®
) laminations
: Yes.
: Yes, if used with paper or Tyvek.
®
: Conditionally.
: No.
716 MEDICAL DEVICE PACKAGING
cases, must facilitate as well as maintain sterility
throughout distribution and handling.
. Sealant compatibility: Compatibility of the materials
and their thermal transitions must be considered so
that they can be efficiently processed.
. Ability to age: Designers must consider the materials
and issues of mass transfer that may impact the
ability of the system to maintain the SBS throughout
the product’s stated life.
. Cost-effective.
Typical materials for thermoformed trays are high-
impact polystyrene (HIPS), polyvinyl chloride (PVC),
XT polymer, acrylonitrile, polycarbonate (PC), and poly-
ethylene terephthalate glycol (PETG). Lids can be manu-
factured from paper, Tyvek
s
, or a film, depending on the
function, sterilization, and sealer characteristics (10).
Flexible Nonformed Pouches. This type of pouch is
commonly used for single-use disposable items such as
gloves, catheters, tubing, adhesive bandages, dressings,
syringes, and so on. Flexible packages tend to provide less
physical protection than the rigid ones (10) and are a
preferred choice for high-volume, low-cost devices. It is a
packaging form that provides: a sterile barrier, the ability
to withstand sterilization, and, if properly designed, easy-
opening features for dispensing. Varying peel pouches can
be run on form-fill-seal machines.
Examples of flexible, nonformed pouches are flat
pouches and gusset pouches. Flat pouches are bags
made from two webs and sealed along the perimeter.
The end seal is usually V-shaped or ‘‘chevron’’ for ease of
opening. Material combinations include: adhesive coated
paper to paper, paper (coated or uncoated) to film, Tyvek
s
(coated or uncoated) to film, coated Tyvek
s
to Tyvek
s
,
and film (coated or uncoated) to film. Foil laminations are
used if additional barrier properties are needed. Pouches
with the right material combination can be sterilized by
all commercial sterilization processes. Pouches manufac-
tured with nonpermeable materials are limited to radia-
tion sterilization or, under controlled-conditions, steam
(10). Gusset pouches are similar to flat pouches except
that one web is gusseted on the sides or the bottom to
accommodate higher-profile products.
Bags and Vented Flexible Packaging. Bags are exten-
sively used in the industry—in particular when low cost
and high profile are required. Early bags were made of
paper; some types of which are still being used today.
Paper bags have the porosity needed for gas and steam
sterilization. On the other hand, paper bags do not offer a
particulate-free opening and they provide poor puncture
resistance. Traditional paper bags have been replaced by
pouches and trays. Plain polyethylene (PE) bags are used
when clean, but not sterile, delivery is necessary. PE bags
have good mechanical properties, but they are not porous
enough to allow simple sterilization. PE has been shown to
be permeable to ethylene oxide (ETO) sterilization with
slow and closely controlled cycles. Vented bags have been
developed to provide a clean, low-cost, high-profile, strong
package and sterilizable container. Vented bags with
single and double vents allow for ETO sterilization of
large-sized kits.
Examples of bags and vented flexible packaging include
paper bags, vented bags, and header bags. Paper bags are
fabricated from a single sheet of surgical paper with
adhesive zone when sealing is needed. They usually
have a back seam and can be gusseted on the sides or
bottom. They can be manufactured on form-fill-seal (FFS)
packaging equipment. Vented bags are made from film;
they have small windows with breathable patches made of
paper or Tyvek
s
. The patch is needed for gaseous ster-
ilization. Header bags are also plastic bags but instead of
having a breathable patch, the top of the bag is designed
with a peelable paper or Tyvek
s
strip running across the
top. Header bags allow for aseptic presentation while
vented bags do not (10).
Package Sealing. The sealing of medical device packa-
ging is critical. Inappropriate sealing can negatively affect
the package integrity. There are two types of seals: weld
and peelable. Weld seals are achieved by heat or ultra-
sonics and produce a joint that is not designed to open.
Peeable seals are achieved with heat and without heat
(cold seals) and are designed to open. Peelable cold seals
are accomplished by applying a cohesive material to both
webs and then a uniform pressure contact. This seal type
cannot be resealed; as a result, it provides a tamper-
evident feature. Peelable heat seals are more complicated
to achieve since they involve exact control over tempera-
ture, time, and pressure.
Sterilization Processes
Medical devices that will be in contact with blood or
internal tissues, other than the gastrointestinal tract or
other mucosa, and devices that deliver parenteral fluids or
drug substances to the same tissues are expected to be
sterile. Sterility is defined as having not more than one
viable microorganism in a million sterilized products
(SAL = 10
6
). A sterile device must keep its sterility until
it is removed from the primary packaging for use on the
patient (11). In the past, manufacturers of sterile medical
devices frequently guaranteed the sterility of the product
until the package was intentionally opened or accidentally
damaged. This approach has changed in recent years. To
maintain package integrity for such unlimited time poses
a real challenge for any combination of materials, packa-
ging forms, and seals. Recently, the European Union
began requiring manufacturers to provide a shelf-life
date and data that support the maintenance of the SBS
throughout the stated timeframe.
Ethylene oxide (EtO) and radiation (gamma and elec-
tron beams) are the two dominant sterilization methods.
As a rule of thumb, if product and packaging can with-
stand radiation, medical device manufacturers tend to use
gamma radiation. If not, then EtO is the choice. Alternate
MEDICAL DEVICE PACKAGING 717